 Haimanot Abebe Adane
Haimanot Abebe Adane Ross Iles1
Ross Iles1- 1School of Public Health and Preventive Medicine, Faculty of Medicine, Nursing and Health Sciences, Monash University, Melbourne, VIC, Australia
- 2Eastern Health Clinical School, Faculty of Medicine, Nursing and Health Sciences, Monash University, Melbourne, VIC, Australia
Objective: This systematic review and meta-analysis aimed to summarize the evidence on the relationship between physical occupational risks (high physical workload, long working hours, shift work, whole-body vibrations, prolonged standing, and heavy lifting) and preterm birth.
Methods: A systematic review and meta-analysis was conducted across six databases to investigate the relationship between physical occupational risks and preterm birth.
Result: A comprehensive analysis of 37 studies with varying sample sizes found moderate evidence of positive associations between high physical workload, long working hours, shift work, whole-body vibration, and preterm birth. Meta-analysis showed a 44% higher risk (OR 1.44, 95% CI 1.25–1.66) for preterm birth with long working hours and a 63% higher risk (OR 1.63, 95% CI 1.03–2.58) with shift work.
Conclusion: Pregnant women in physically demanding jobs, those working long hours or on shifts, and those exposed to whole-body vibration have an increased risk of preterm birth. Employers should establish supportive workplaces, policymakers implement protective measures, healthcare providers conduct screenings, and pregnant women must stay informed and mitigate these job-related risks.
Systematic Review Registration: [https://www.crd.york.ac.uk/prospero/], Identifier [CRD42022357045].
Introduction
The World Health Organization (WHO) defines preterm birth as the birth of a baby before 37 weeks of pregnancy [1]. Rates of preterm birth range from 5% to 18% across 184 nations [2]. An estimated 15 million preterm births occur worldwide each year, with 1.1 million infant deaths as a result of preterm birth, making it one of the leading causes of mortality in children under 5 years of age [3]. Preterm birth can cause short- and long-term health problems for children, such as diabetes, high blood pressure, and heart disease later in life [4–6]. Most preterm births are spontaneous, but around 30% are provider-initiated, involving induction or primary cesarean section, termed medically indicated [7].
The global workforce has seen a significant increase in the participation of pregnant women [8]. In the European Union, two-thirds of women of working age or older were employed in 2020 [9]. Over 40% of women in Europe worked in physically demanding jobs, 21% worked rotating shifts, 15% worked more than 40 h per week, and 14% worked night shifts [9]. In many lower and middle-income countries, the employment rate of women is also high, at 32.17% [10]. However, the vast majority of women who work in the paid economy are in the informal economy [10]. The increasing number of reproductive-age women in paid employment raises concerns about the impact on pregnancy outcomes [11]. Previous studies have shown that pregnant working women are at increased risk of poor maternal and newborn health, including preterm birth [12–14].
Preterm birth is most commonly caused by factors such as multiple pregnancies, infections, and chronic health conditions [15]. However, there is growing evidence that occupational factors, such as physically demanding work, whole-body vibration, long hours, and shift work, may also increase the risk of preterm birth [16–18]. For example, a systematic review of studies found that women who worked long hours were more likely to have a preterm birth [18]. Another review found that pregnant women who worked long hours while standing, lifting heavy objects, or working shifts or nights were also at increased risk [16, 19].
While the evidence from these reviews is useful, their authors report conflicting or weak evidence and as such have concluded that it is challenging to provide explicit recommendations for clinical practice or policy [12, 16, 18]. Some limitations of these prior reviews include not reporting on study quality [12, 20], none have examined the impacts of whole-body vibration on preterm birth, and none have sought to differentiate between medically indicated or spontaneous preterm birth [16, 17, 20]. Further, the included evidence in most reviews reflect working conditions of the late 20th century, up to the early 2000’s [16, 21]. In many occupations and nations, working conditions have changed dramatically throughout the early 21st century and thus the nature, prevalence and impacts of occupational physical health risks has also changed [22, 23].
Pregnant women are often exposed to physical occupational risks, such as high physical workload, heavy lifting, long working hours, long-standing hours, and shift work [22]. These risks are common, have a significant impact on reproductive health [23], and are more modifiable than chemical and biological exposures [21]. This systematic review and meta-analysis was conducted to investigate the relationship between physical occupational risks and preterm birth. A better understanding of this relationship has been gained and is helpful for obstetricians, occupational health services, employers, and policymakers in developing strategies to reduce the risk of preterm birth.
Methods
This systematic review and meta-analysis was reported in accordance with PRISMA guidelines [24]. The study protocol was registered with PROSPERO (CRD42018094400) and published in PLOS One [25].
Search Strategy
Six electronic databases were searched without geographic restrictions to identify studies examining the effects of exposure to physical occupational risks, such as physically demanding work, long working hours, shift work, whole-body vibration, prolonged standing, and heavy lifting on preterm birth in paid employed pregnant women. A broad range of potential search terms, including Medical Subject Headings (MeSH) terms and keywords (as shown in Supplementary Table S1), were employed for the search. Additionally, the reference lists of the included studies were examined to identify relevant research.
Eligibility Criteria
This review included original research studies that examined the link between physical occupational risks and preterm birth in pregnant women who were employed during pregnancy. Studies were observational (prospective, retrospective, case-control, cross-sectional) or interventional designs. Studies were excluded if they were reviews, case studies, qualitative studies, editorials, commentaries, conference abstracts, or unpublished manuscripts; published in languages other than English, before the year 2000, and investigated the effect of non-physical occupational risks, such as biological, chemical, or psychosocial hazards.
Outcome
The primary outcome of interest was preterm birth, defined as babies born alive less than 37 weeks of pregnancy [1]. We also examined different types of preterm birth as secondary outcomes, including extremely preterm birth (<28 weeks), very preterm birth (28-<32 weeks), moderate preterm birth (32-<37 weeks), and spontaneous birth (delivery onset by spontaneous labor or premature rupture of membranes) or medically indicated birth (delivery onset through induction or primary caesarean section) [7].
Exposure
Six of the most commonly prevalent physical occupational risks were identified as the exposure of interest. These were high physical workload, long working hours, shift work, whole-body vibrations prolonged standing, and heavy lifting. Due to a wide variation in exposure definitions in the literature, we adopted broad definitions to ensure that all articles reporting relevant exposures were captured (See Table 1).
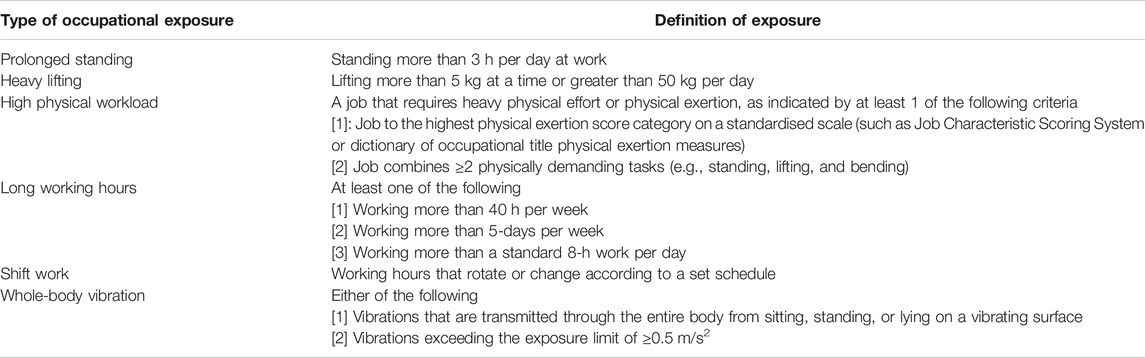
TABLE 1. Definition of physical occupational risks (Australia, 2023).
Study Selection
All articles found from electronic databases and reference chaining were gathered in EndNote. Duplicate articles were removed, and the remaining articles were imported into Covidence. Two independent reviewers screened the titles and abstracts of all articles against eligibility criteria (HAA and AG). Articles on which both reviewers agreed were excluded or progressed to the next stage. Disagreements were resolved by consensus or a third reviewer (RI). The full text of all articles that passed the initial screening was retrieved and assessed for eligibility by two independent reviewers. Again, disagreements were resolved by consensus or a third reviewer.
Data Extraction
Data were extracted from all included studies by two independent reviewers using a standard data extraction tool. The following information was extracted: study characteristics (study period, study design, country), population characteristics (number of participants), type of exposure, gestational time women engaged in work (exposure timing), method of exposure assessment, outcome (preterm birth and subtype), confounders considered, effect estimates, and main finding.
Risk of Bias (ROB) Assessment
The risk of bias of the included studies was assessed using tools from the Joanna Briggs Institute (JBI) [26]. These tools assessed the quality of different types of studies for potential sources of bias, such as inappropriate sampling, measurement, outcomes, confounding factors, and statistical analysis. The quality assessment was conducted independently by two reviewers (HAA and AG). In cases where there was a discrepancy, a third reviewer (RI) was consulted to achieve consensus. A study was deemed to have a low risk of bias if more than 70% of responses were marked as “yes,” a moderate risk of bias if between 50% and 69% of responses were marked as “yes,” and a high risk of bias if less than 50% of responses were marked as “yes” [27]. Studies with a high risk of bias were excluded from further synthesis and analysis.
Evidence Synthesis
We used the GRADE (Grading of Recommendations, Assessment, Development, and Evaluation) method to assess the quality of evidence for each exposure and outcome [28]. The certainty of evidence was rated high, moderate, low, or very low. We started with a high rating for RCTs and a low rating for observational studies. The certainty of evidence from observational studies may be downgraded if two or more of the following five factors are present: risk of bias, indirectness, inconsistency, imprecision, and publication bias. Risk of bias across studies was rated as serious when ≥50% of the eligible studies had high ROB, otherwise it was considered as not serious. Indirectness was rated as serious when ≥50% of the eligible studies had significant differences in the population, exposure or outcomes examined, otherwise it was considered as not serious. Inconsistency was rated as serious when ≥50% of the eligible studies had a large variation in the effect estimate, otherwise it was considered as not serious. Imprecision was rated as serious if ≥ 50% of the eligible studies did not meet optimal information size (OIS) criteria (i.e., if the total number of populations included in the SLR is less than the number of populations generated by a conventional sample size calculation for a single study adequately powered trial), and if OIS was met and the 95% CI overlaps no effect, otherwise it was considered as not serious. Publication bias was rated serious if the eligible studies only included large sample size (≥2000), only reported positive results, and search strategies were believed to be less comprehensive. Otherwise it was considered as not serious. The certainty assessment could also be up-rated if one of three domains were observed (large magnitude of effect, evidence of a dose-response relationship, and counteracting plausible residual bias). The GRADE method was used to develop practical guidance from the evidence [29]. Recommendations were made based on how confident we were in the evidence. High-quality evidence led to strong recommendations, moderate-quality evidence led to practice considerations, and low-quality evidence meant that there was not enough evidence to guide policymakers, clinicians, and patients.
Meta-Analysis
Meta-analyses were performed using the generic inverse variance method with random effects modelling if there were sufficient studies with a similar definition of exposure and outcomes of interest. We calculated a pooled odds ratio (OR) with a 95% confidence interval (CI) for the primary outcome. Visual inspection of forest plots and I2 statistics tests were used to assess heterogeneity between studies. Publication bias was investigated using the Egger’s weighted regression test and the Begg’s test. The meta-analysis was conducted using Stata V17 (Stata/SE, Windows, macOS, Linux).
Results
Search Result
In the initial search, 3,712 records were identified (See Figure 1). After removing duplicates, screening the title, abstracts and full text, 36 studies were included. One additional study was added from 17 other records identified from the reference lists of included studies. Thus, a total of 37 articles proceeded to data extraction and quality assessment.
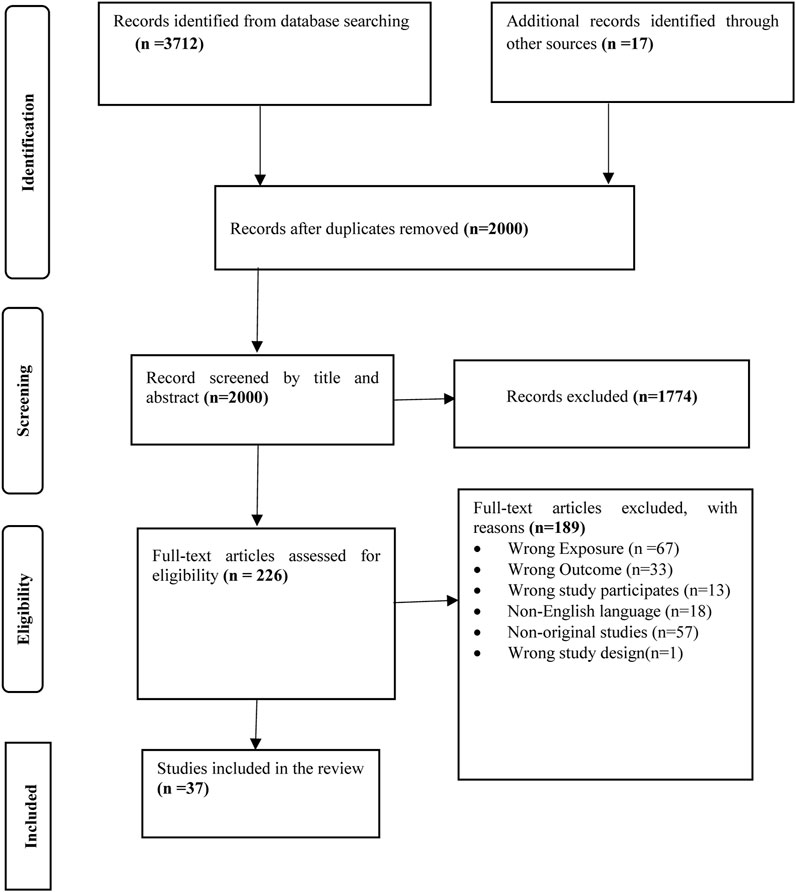
FIGURE 1. PRISMA flow diagram of searching, screening, and sorting (Australia, 2023).
Characteristics of the Included Studies
Country of Origin
Table 2 presents the summary of the study characteristics of the 37 included studies. There were 29 studies from high income countries, including 18 studies from Europe [30–47], seven studies from the United States [48–54], two studies from Asia [55, 56] and one each from Australia [57] and Canada [58]. There were fewer (n = 8) studies conducted in low-income countries, including four each from Africa [59–62] and Asia [63–66].
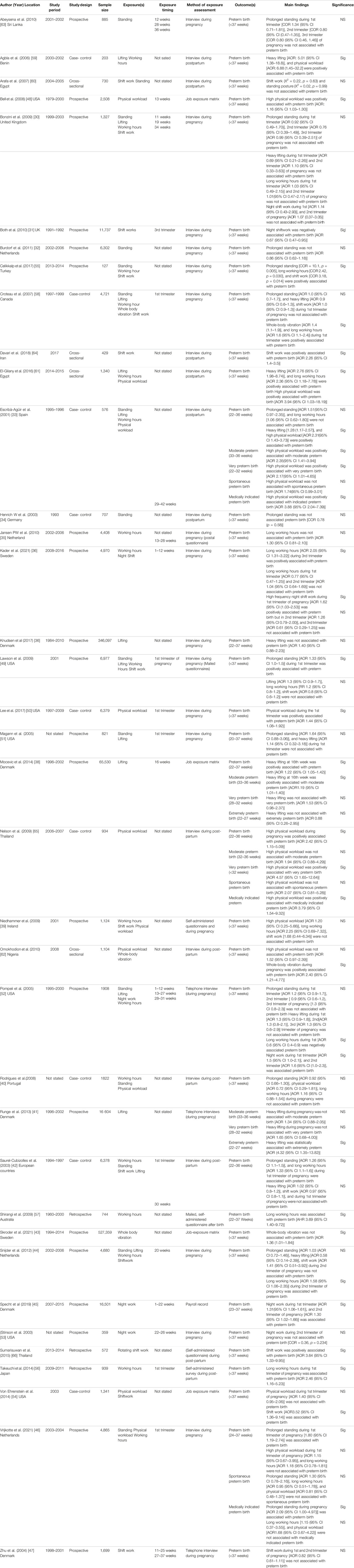
TABLE 2. Details of included studies from 1 January 2000–September 2022 (Australia, 2023).
Study Design
Of the included studies, twenty-one studies were prospective [30–32, 35–39, 41, 43–49, 51–53, 55, 63], nine studies were case control [33, 34, 40, 42, 50, 54, 58, 59, 65], three studies were retrospective [56, 57, 66], and four cross-sectional studies [60–62, 64]. In 21 cohort investigations [30–32, 35–39, 41, 43–49, 51–53, 55, 63] exposure was ascertained prospectively during pregnancy, whereas for 16 studies [33, 34, 40, 42, 50, 54, 56–62, 64–66] (nine case-control, three retrospective cohort, and four cross-sectional studies), information about exposure was elicited after the relevant birth outcome had occurred.
Exposure Assessment and Sample Size
The data on exposure were collected mostly through self-report (by telephone or interview and mail), but in some studies job title was used as surrogate index of exposure [31, 38, 43, 45, 48, 54]. Of the included studies, 19 examined a single exposure [31, 32, 34, 35, 37, 38, 41, 43, 45, 47, 48, 50, 53, 56, 57, 63–66], six examined two exposures [36, 51, 54, 59, 60, 62], five examined three exposures [39, 40, 46, 55, 61], six examined four exposures [31, 33, 42, 44, 49, 52], and one examined five exposures [58]. Eight studies also reported the time of exposure as being during the 1st trimester, three studies at 2nd trimester, one study at 3rd trimester, five studies at all trimester, one study both at 2nd and 3rd trimester and the remaining 20 studies did not state the exposure timing by trimester. The included studies involved 1,054,008 participants with sample size ranging from 127 to 527,359 participants [43, 55].
Outcome
Except for two studies, preterm birth was determined using hospital records, registers, or birth certificates [55, 66]. All but nine of the studies used the World Health Organization’s definition of preterm birth, which is the birth of a live fetus before 37 completed weeks of pregnancy [33, 37, 38, 41, 42, 45, 46, 57, 65].
Methodological Risk of Bias Assessment
Methodological risk of bias assessment was conducted on thirty-seven studies, 27 were classified as having low-risk of bias [30–33, 35–38, 41–46, 48, 50–52, 56–59, 61, 62, 64–66], two were classified as having moderate risk of bias [54, 55], and eight were classified as having high risk of bias [34, 39, 40, 47, 49, 53, 60, 63] (See Supplementary Material S2).
Potential Cofounding Factors
Thirty-two studies controlled for potential confounding factors using various methods, including matching, restriction, stratification, and multivariate regression modeling. However, five studies did not address confounding at all [34, 53, 59, 60, 63]. Of the 32 studies including statistical adjustment for confounding, maternal age was the most commonly adjusted for variable, in 29 studies [32, 33, 35–52, 54–58, 61, 62, 65, 66] followed by maternal education (n = 22 studies) [30–33, 35, 36, 40–44, 46, 48–52, 54, 58, 61, 62, 65], parity (number of live births) (n = 20 studies) [30–32, 35–37, 39–41, 44–46, 48, 49, 52, 56, 58, 61, 62, 65], maternal smoking (n = 15 studies) [35–39, 42–47, 50, 52, 56] and hypertension during pregnancy [33, 42, 43, 49, 50, 54, 58, 62] (n = 8 studies). Of the five studies not using statistical adjustment, four used the Chi-square test to examine association between exposure and outcome [34, 53, 55, 60].
Certainty Assessment (GRADE)
The overall certainty of evidence ranged from very low to moderate for each of the six exposure categories (See Supplementary Table S3). All the included studies were observational studies, and thus started as low-certainty assessments. The most common reasons for downgrading the certainty of evidence were [1] indirectness [2], imprecision and [3] inconsistency (n = 1). On the other hand, the most common reason for uprating certainty was large effect size and adjustment for plausible cofounding. Although observational studies started as low certainty evidence, we found a moderately certain evidence for the exposure categories physical workload, working hours, shift work, whole-body vibration, which were rated up. On the other hand, due to indirectness and impression, the certainty of evidence was downgraded into very-low evidence for the exposure categories prolonged standing and heavy lifting. There was no evidence of publication bias within the included studies.
The Relation Between Physical Occupational Risks and Preterm Birth
Physical Workload
Ten of the included studies investigated the relationship between physical workload and preterm birth [33, 39, 40, 46, 48, 50, 54, 61, 62, 65]. Two studies with a higher risk of bias were excluded from further analysis [39, 40]. Of the remaining eight high-quality studies, six found a statistically significant positive association between physical workload and preterm birth [33, 48, 50, 54, 61, 65], while the other two did not find such a relationship [46, 62]. Overall, there is moderate evidence that physical workload is associated with an increased risk of preterm birth. However, due to differences in how physical workload was measured across the studies, it was not possible to calculate a precise estimate of the effect of physical workload on preterm birth.
Working Hours
Sixteen studies analysed the relationship between long working hours and preterm birth [30, 33, 35, 36, 39, 40, 42, 44, 46, 49, 52, 55–58, 61]. Three studies had high ROB, and thus were excluded in further synthesis and meta-analysis [39, 40, 49]. Six low ROB [36, 42, 55–58, 61] and one moderate ROB studies [55] reported a positive statistically significant association between long working hours and preterm birth. One study found a negative relationship [52] and five studies showed no statistical association between working hours and preterm birth [30, 33, 35, 44, 46]. The overall finding was moderate evidence of a positive association between long working hours and preterm birth. Six low ROB studies were feasible to combine in formal meta-analysis on the relationship between working hours (>40 h/day vs. less) and preterm birth. The pooled effect estimate based on four studies was 1.44 (1.25–1.66) (see Figure 2).
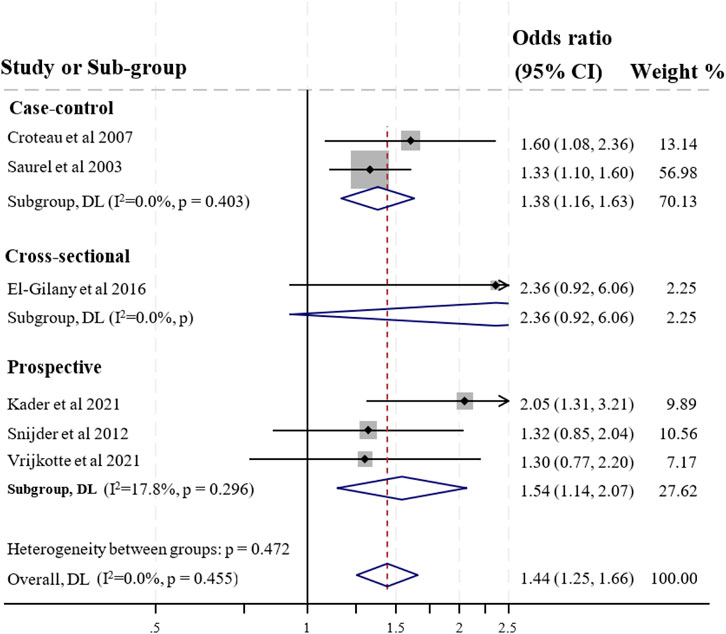
FIGURE 2. Forest plot for preterm birth and working >40 h per week during pregnancy (Australia, 2023).
Shift Work
The relationship between shiftwork and pre-term birth was examined in fifteen studies [31, 36, 39, 44, 45, 47, 49, 52–55, 58, 60, 64, 66]. Five studies with high ROB were excluded from further synthesis and meta-analysis [39, 47, 49, 53, 60]. The remaining four studies with low ROB [36, 52, 64, 66] and two study with moderate ROB [54, 55] showed a positive relationship between shift work and preterm birth. One study showed that working night shift in the third trimester of pregnancy was protective for the occurrence of preterm birth [31]. Three studies reported no association between shift work and preterm birth [44, 45, 58]. Hence, the overall result showed a moderate evidence of a positive statistically significant association between shift work and preterm birth. Of ten studies, four studies with low ROB were feasible to include in a formal meta-analysis on the relationship between shift work or night work (Yes vs. No) and preterm birth. The pooled effect estimate based on four studies was 1.63 (1.03–2.58) (see Figure 3).
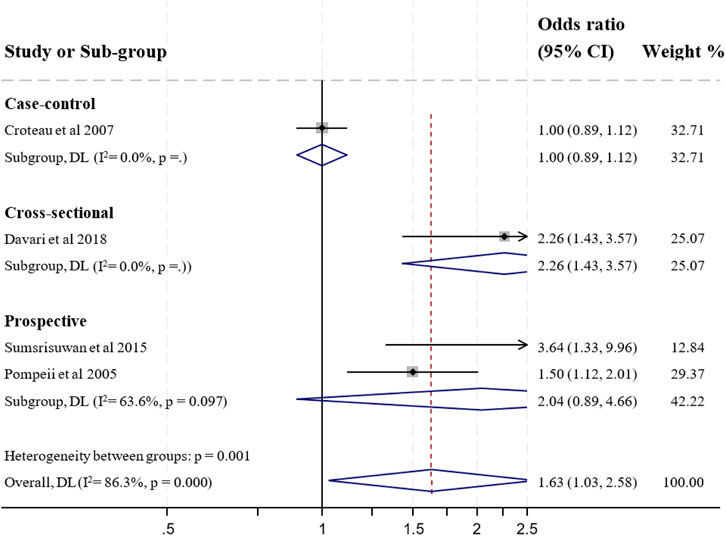
FIGURE 3. Forest plot for preterm birth and shift work during pregnancy (Australia, 2023).
Whole-Body Vibration (WBV)
The relationship between whole-body vibration and preterm birth was assessed in three studies all of which were rated as having low ROB [43, 58, 62]. All of these studies reported a positive statistically significant association between whole-body vibration and preterm birth [43, 58, 62]. The overall finding showed moderate evidence of a positive statistical association between whole-body vibration and increased odds of preterm birth. Due to exposure definition differences, meta-analysis was not possible.
Standing
Of the included studies, fourteen studies examined the relationship between standing and preterm-birth [30, 32–34, 42, 44, 46, 49, 51, 52, 55, 58, 60, 63]. Four studies had high risk of bias and thus were excluded from further synthesis and meta-analysis [34, 49, 60, 63]. Of the included studies for further synthesis, two low ROB studies [30, 46] and one moderate ROB study described a positive statistically significant relationship between prolonged standing and pre-term birth [55]. The remaining seven low ROB studies did not find a statistically significant relationship between prolonged standing and preterm birth [30, 32, 33, 44, 51, 52, 58]. Overall these findings indicate very low evidence of no statistically significant association between prolonged standing and preterm birth. Because of discrepancies in defining exposure, conducting a meta-analysis for prolonged standing and preterm birth was impossible.
Lifting
Twelve studies examined the relationship between lifting and preterm birth [30, 33, 37, 38, 42, 44, 49, 51, 52, 58, 59, 61], of which 11 studies had low risk of bias [30, 33, 37, 38, 42, 44, 51, 52, 58, 59, 61]. One study had high risk of bias and thus was excluded from further synthesis [49]. Four of the elven included studies found a positive statistically significant relationship between lifting and preterm birth [33, 38, 59, 61]. The remaining seven studies did not find a statistically significant association between lifting and preterm birth [30, 37, 42, 44, 51, 52, 58]. Overall, findings indicated very low evidence of no statistically significant association between heavy lifting and preterm birth. Due to disparities in the definition of exposure, conducting a meta-analysis for heavy lifting and preterm birth was rendered infeasible.
Secondary Outcomes: Type of Pre-term Birth
Three low ROB studies examined the relationship between physical workload and medically indicated preterm birth and/or spontaneous preterm birth [33, 46, 65]. Two of the three studies reported a positive statistically significant association between high physical workload and medically indicated preterm birth [33, 65], suggesting moderate evidence of a relationship. However, all three studies reported no statistical association between high physical workload and spontaneous preterm birth [33, 46, 65], providing moderate evidence of no association. Two low ROB studies examined the relationship between physical workload and very preterm birth or moderate preterm birth [33, 65]. Both reported a positive statistically significant association with very pre-term birth providing moderate evidence of an association [33, 65]. One study showed a positive association between high physical workload and moderate preterm birth, providing inconclusive evidence of a relationship [33]. Two low ROB studies investigated the relationship between heavy lifting and moderate preterm birth, very preterm birth [38, 41], and extremely preterm birth. Both reported no association between heavy lifting and moderate preterm birth and very preterm birth [38, 41]. However, a single study reported a positive statistical association between heavy lifting and extremely preterm birth, providing inconclusive evidence [41].
Discussion
A systematic review and meta-analysis found that physical occupational risk factors during pregnancy are associated with an increased risk of preterm birth. Preterm birth is a serious pregnancy complication linked to long-term neurodevelopmental problems and chronic health conditions in children [67, 68]. This review found moderate evidence that high physical workload, long working hours, shift work, and whole-body vibration during pregnancy increase the risk of preterm birth. It also found that high physical workload may contribute to medically indicated and very preterm birth. However, there are gaps in the evidence base on the association of physical occupational risks and preterm birth, suggesting opportunities for future research.
Although it is challenging to demonstrate a causal relationship between physical occupational exposures and adverse perinatal outcomes (preterm birth) due to the observational nature of these studies, there are plausible potential physiological mechanisms for this association. These include that high physical workload, long working hours, shift work and whole-body vibration may cause fatigue [69], stress, sleep deprivation, and circadian rhythm disruption [70, 71], this result increased release of catecholamine [72], increased prostaglandins production [73] and corticosterone level [74] which may increase uterine contractility and decrease placental function [75]. This could in turn lead to preterm birth. It could also be that women who work in physically demanding jobs, long working hours, shift work, and whole-body vibrations are also exposed to other occupational risks, social, psychological, life style or environmental risk factors for pre-term birth that are not accounted for in these observational studies (i.e., unobserved confounding) [76–79]. For example women in physically demanding jobs may also have lower incomes than those in “white collar” jobs (professional, office-based, or administrative occupations), which may affect multiple determinants of maternal and neonatal health such as nutrition and access to healthcare [80]. Some studies in this review took socioeconomic factors into account, but most did not consider other common occupational risks that may be interconnected. It is important to comprehensively understand how these occupational risks, such as psychosocial work factors, can contribute to preterm birth. This finding suggests that preterm birth may be preventable in some working women by reducing their exposure to heavy physical workloads, long working hours, shift work, and whole-body vibrations. Pregnant women should be aware of the risks associated with these occupational risks and take steps to minimize their exposure. Employers and regulatory authorities have a responsibility to create policies and work practices that reduce the exposure of pregnant women to these hazards.
This systematic review also identified moderate evidence of a positive association between high physical workload and medically indicated and very-preterm birth [33, 65]. There may be biological mediators that explain this relationship like the presence of hypertriton during pregnancy [81]. For example, women in the Canada who experienced physical workload and pre-eclampsia had greater risk of medically indicated preterm birth and very preterm birth [82, 83]. Hence, high physical demanding jobs potentially increases the risk of or pre-eclampsia and more likely to have a medically indicated preterm birth. The results indicate that a need to separate preterm births into subcategories to properly evaluate the relationship between high physical workload and preterm births.
In this systematic review we found a large number of studies on the relationship between physical occupational risks and preterm birth from developed countries and very few studies from low-income countries [48, 55, 56, 59–62, 64–66] though there are many babies born preterm in these regions (9.3% vs. 12%) respectively [68]. Female labor force participation is notably high in both low-income and high-income countries worldwide, with significant shifts in job characteristics over the past decades [84]. Similarly, substantial progress has been achieved in maternal and child healthcare services in recent decades, although maternal and neonatal mortality rates continue to remain high [85]. Majority of the included studies had collated data and published before 2000 and 2013 respectively [30–35, 39, 40, 42, 44, 47–49, 51–53, 57–60, 62, 63, 65]. There is a lack of recent evidence on how the changing nature of jobs and occupational exposures affect pregnant women and their babies. Researchers need to study the link between occupational exposures (such as psychosocial job strain, working hours, and shift work) and preterm birth. There is also a need for employers to consider modifying the physical working environment and working conditions for pregnant women to reduce the risk of preterm birth and other negative birth outcomes.
Strengths and Limitations of This Review
This review’s strength lies in its rigorous methodology, including risk assessment and GRADE synthesis. It uniquely focuses on working pregnant women, avoiding potential bias introduced by comparing them with unemployed individuals. This approach ensures greater relevance to the target audience and enhances the review’s credibility [86, 87]. To minimize bias, this review exclusively considered studies involving employed women in both exposure and control groups. However, it has limitations, including the restriction to English-language articles, potentially missing studies in other languages. Additionally, reliance on data solely from observational studies increased result heterogeneity and reduced evidence certainty. Most studies assessed occupational physical exposures through self-reported measures, potentially introducing recall bias.
Conclusion
This systematic review and meta-analysis found that working in physically demanding jobs, long hours, shift work, and jobs that expose women to whole-body vibration increase the chance of having preterm birth. Further research is needed to investigate the effect of occupational risks on preterm birth among employed pregnant women, using a follow-up design and evidence synthesis.
Author Contributions
HA, RI, JB, AG, and AC contributed to the conception or design, analysis and interpretation of data from the work. HA and AG screened and extracted the data. HA drafted the first manuscript. All authors contributed to the interpretation of the result, critically reviewed the manuscript, and provided important intellectual content.
Funding
AC is supported by an Australian Research Council Future Fellowship (FT190100218). HA is supported by a Monash graduate scholarship.
Conflict of Interest
The authors declare that they do not have any conflicts of interest.
Acknowledgments
The authors thank the Alfred Ian Potter research and training librarian, Lorena Romero for their support in developing the search strategy.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.ssph-journal.org/articles/10.3389/phrs.2023.1606085/full#supplementary-material
References
1. WHO. World Health Statistics: A Snapshot of Global Health. Geneva: Organización Mundial de la Salud (2012).
2. WHO. World Health Statistics 2017: Monitoring Health for the SDGs. sustainable development goals (2017).
3. Purisch, SE, and Gyamfi-Bannerman, C. Epidemiology of Preterm Birth. Semin Perinatol (2017) 41(7):387–91. doi:10.1053/j.semperi.2017.07.009
4. Bensley, JG, De Matteo, R, Harding, R, and Black, MJ. The Effects of Preterm Birth and its Antecedents on the Cardiovascular System. Acta obstetricia gynecologica Scand (2016) 95(6):652–63. doi:10.1111/aogs.12880
5. Luu, TM, Mian, MOR, and Nuyt, AM. Long-Term Impact of Preterm Birth: Neurodevelopmental and Physical Health Outcomes. Clin perinatology (2017) 44(2):305–14. doi:10.1016/j.clp.2017.01.003
6. Soleimani, F, Zaheri, F, and Abdi, F. Long-Term Neurodevelopmental Outcomes After Preterm Birth. Iranian Red Crescent Med J (2014) 16(6):e17965. doi:10.5812/ircmj.17965
7. Moutquin, JM. Classification and Heterogeneity of Preterm Birth. BJOG: Int J Obstet Gynaecol (2003) 110:30–3. doi:10.1016/s1470-0328(03)00021-1
8. Figà-Talamanca, I. Occupational Risk Factors and Reproductive Health of Women. Occup Med (2006) 56(8):521–31. doi:10.1093/occmed/kql114
10. Ortiz-Ospina, E, Tzvetkova, S, and Roser, M. Women’s Employment: Our World in Data (2018). Available from: https://ourworldindata.org/female-labor-supply (Accessed September 15, 2023).
11. Quansah, R, and Jaakkola, JJ. Occupational Exposures and Adverse Pregnancy Outcomes Among Nurses: A Systematic Review and Meta-Analysis. J women's Health (2010) 19(10):1851–62. doi:10.1089/jwh.2009.1876
12. Bonzini, M, Coggon, D, and Palmer, KT. Risk of Prematurity, Low Birthweight and Pre-Eclampsia in Relation to Working Hours and Physical Activities: A Systematic Review. Occup Environ Med (2007) 64(4):228–43. doi:10.1136/oem.2006.026872
13. Mutambudzi, M, Meyer, JD, Warren, N, and Reisine, S. Effects of Psychosocial Characteristics of Work on Pregnancy Outcomes: A Critical Review. Women & health (2011) 51(3):279–97. doi:10.1080/03630242.2011.560242
14. Pak, VM, Powers, M, and Liu, J. Occupational Chemical Exposures Among Cosmetologists: Risk of Reproductive Disorders. Workplace Health Saf (2013) 61(12):522–8. doi:10.1177/216507991306101204
15. Bizuayehu, HM, Harris, ML, Chojenta, C, Forder, PM, and Loxton, D. Biopsychosocial Factors Influencing the Occurrence and Recurrence of Preterm Singleton Births Among Australian Women: A Prospective Cohort Study. Midwifery (2022) 110:103334. doi:10.1016/j.midw.2022.103334
16. Cai, C, Vandermeer, B, Khurana, R, Nerenberg, K, Featherstone, R, Sebastianski, M, et al. The Impact of Occupational Activities During Pregnancy on Pregnancy Outcomes: A Systematic Review and Metaanalysis. Am J Obstet Gynecol (2020) 222(3):224–38. doi:10.1016/j.ajog.2019.08.059
17. Croteau, A. Occupational Lifting and Adverse Pregnancy Outcome: A Systematic Review and Meta-Analysis. Occup Environ Med (2020) 77(7):496–505. doi:10.1136/oemed-2019-106334
18. Van Melick, M, Van Beukering, M, Mol, BW, Frings-Dresen, M, and Hulshof, C. Shift Work, Long Working Hours and Preterm Birth: A Systematic Review and Meta-Analysis. Int Arch Occup Environ Health (2014) 87:835–49. doi:10.1007/s00420-014-0934-9
19. Cai, C, Vandermeer, B, Khurana, R, Nerenberg, K, Featherstone, R, Sebastianski, M, et al. The Impact of Occupational Shift Work and Working Hours During Pregnancy on Health Outcomes: A Systematic Review and Meta-Analysis. Am J Obstet Gynecol (2019) 221(6):563–76. doi:10.1016/j.ajog.2019.06.051
20. Van Beukering, M, Van Melick, M, Mol, BW, Frings-Dresen, M, and Hulshof, C. Physically Demanding Work and Preterm Delivery: A Systematic Review and Meta-Analysis. Int Arch Occup Environ Health (2014) 87:809–34. doi:10.1007/s00420-013-0924-3
21. Palmer, KT, Bonzini, M, Harris, EC, Linaker, C, and Bonde, JP. Work Activities and Risk of Prematurity, Low Birth Weight and Pre-Eclampsia: An Updated Review With Meta-Analysis. Occup Environ Med (2013) 70(4):213–22. doi:10.1136/oemed-2012-101032
22. García, AM, González-Galarzo, MC, Ronda, E, Ballester, F, Estarlich, M, Guxens, M, et al. Prevalence of Exposure to Occupational Risks During Pregnancy in Spain. Int J Public Health (2012) 57:817–26. doi:10.1007/s00038-012-0384-7
23. Razafimahefa, RH, Pardosi, JF, and Sav, A. Occupational Factors Affecting Women Workers’ Sexual and Reproductive Health Outcomes in Oil, Gas, and Mining Industry: A Scoping Review. Public Health Rev (2022) 43:1604653. doi:10.3389/phrs.2022.1604653
24. Page, MJ, McKenzie, JE, Bossuyt, PM, Boutron, I, Hoffmann, TC, Mulrow, CD, et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. BMJ (2021) 372:n71. doi:10.1136/bmj.n71
25. Adane, HA, Iles, R, Boyle, JA, and Collie, A. Maternal Occupational Risk Factors and Preterm Birth: Protocol for a Systematic Review and Meta-Analysis. Plos one (2023) 18(7):e0283752. doi:10.1371/journal.pone.0283752
26. Peters, MD, Godfrey, C, McInerney, P, Munn, Z, Tricco, A, Khalil, H, et al. JBI Manual for Evidence Synthesis (2020). Available from: https://jbi-global-wiki.refined.site/space/MANUAL (Accessed September 16, 2023).
27. Mruts, K, Tessema, G, Gebremedhin, A, Scott, J, and Pereira, G. The Effect of Family Planning Counselling on Postpartum Modern Contraceptive Uptake in Sub-Saharan Africa: A Systematic Review. Public Health (2022) 206:46–56. doi:10.1016/j.puhe.2022.02.017
28. Guyatt, GH, Oxman, AD, Kunz, R, Woodcock, J, Brozek, J, Helfand, M, et al. GRADE Guidelines: 8. Rating the Quality of Evidence—Indirectness. J Clin Epidemiol (2011) 64(12):1303–10. doi:10.1016/j.jclinepi.2011.04.014
29. Granholm, A, Alhazzani, W, and Møller, MH. Use of the GRADE Approach in Systematic Reviews and Guidelines. Br J Anaesth (2019) 123(5):554–9. doi:10.1016/j.bja.2019.08.015
30. Bonzini, M, Coggon, D, Godfrey, K, Inskip, H, Crozier, S, and Palmer, KT. Occupational Physical Activities, Working Hours and Outcome of Pregnancy: Findings From the Southampton Women's Survey. Occup Environ Med (2009) 66(10):685–90. doi:10.1136/oem.2008.043935
31. Both, MI, Overvest, MA, Wildhagen, MF, Golding, J, and Wildschut, HI. The Association of Daily Physical Activity and Birth Outcome: A Population-Based Cohort Study. Eur J Epidemiol (2010) 25(6):421–9. doi:10.1007/s10654-010-9458-0
32. Burdorf, A, Brand, T, Jaddoe, VW, Hofman, A, Mackenbach, JP, and Steegers, EA. The Effects of Work-Related Maternal Risk Factors on Time to Pregnancy, Preterm Birth and Birth Weight: The Generation R Study. Occup Environ Med (2011) 68(3):197–204. doi:10.1136/oem.2009.046516
33. Escriba-Aguir, V, Perez-Hoyos, S, and Saurel-Cubizolles, MJ. Physical Load and Psychological Demand at Work During Pregnancy and Preterm Birth. Int Arch Occup Environ Health (2001) 74(8):583–8. doi:10.1007/s004200100259
34. Henrich, W, Schmider, A, Fuchs, I, Schmidt, F, and Dudenhausen, JW. The Effects of Working Conditions and Antenatal Leave for the Risk of Premature Birth in Berlin. Arch Gynecol Obstet (2003) 269(1):37–9. doi:10.1007/s00404-003-0487-8
35. Jansen, PW, Tiemeier, H, Verhulst, FC, Burdorf, A, Jaddoe, VW, Hofman, A, et al. Employment Status and the Risk of Pregnancy Complications: The Generation R Study. Occup Environ Med (2010) 67(6):387–94. doi:10.1136/oem.2009.046300
36. Kader, M, Bigert, C, Andersson, T, Selander, J, Bodin, T, Skroder, H, et al. Shift and Night Work During Pregnancy and Preterm Birth-A Cohort Study of Swedish Health Care Employees. Int J Epidemiol (2022) 50(6):1864–74. doi:10.1093/ije/dyab135
37. Knudsen, IR, Bonde, JP, and Petersen, SB. Physically Strenuous Work during Pregnancy and Risk of Preterm Birth. Arch Environ Occup Health (2018) 73(4):236–42. doi:10.1080/19338244.2017.1342589
38. Mocevic, E, Svendsen, SW, Jorgensen, KT, Frost, P, and Bonde, JP. Occupational Lifting, Fetal Death and Preterm Birth: Findings From the Danish National Birth Cohort Using a Job Exposure Matrix. PLoS One (2014) 9(3):e90550. doi:10.1371/journal.pone.0090550
39. Niedhammer, I, O'Mahony, D, Daly, S, Morrison, JJ, and Kelleher, CC, Lifeways Cross-Generation Cohort Study Steering Group. Occupational Predictors of Pregnancy Outcomes in Irish Working Women in the Lifeways Cohort. BJOG (2009) 116(7):943–52. doi:10.1111/j.1471-0528.2009.02160.x
40. Rodrigues, T, and Barros, H. Maternal Unemployment: An Indicator of Spontaneous Preterm Delivery Risk. Eur J Epidemiol (2008) 23(10):689–93. doi:10.1007/s10654-008-9283-x
41. Runge, SB, Pedersen, JK, Svendsen, SW, Juhl, M, Bonde, JP, and Nybo Andersen, AM. Occupational Lifting of Heavy Loads and Preterm Birth: A Study Within the Danish National Birth Cohort. Occup Environ Med (2013) 70(11):782–8. doi:10.1136/oemed-2012-101173
42. Saurel-Cubizolles, MJ, Zeitlin, J, Lelong, N, Papiernik, E, Di Renzo, GC, Breart, G, et al. Employment, Working Conditions, and Preterm Birth: Results From the Europop Case-Control Survey. J Epidemiol Community Health (2004) 58(5):395–401. doi:10.1136/jech.2003.008029
43. Skroder, H, Pettersson, H, Norlen, F, Gustavsson, P, Rylander, L, Albin, M, et al. Occupational Exposure to Whole Body Vibrations and Birth Outcomes - A Nationwide Cohort Study of Swedish Women. Sci Total Environ (2021) 751:141476. doi:10.1016/j.scitotenv.2020.141476
44. Snijder, CA, Brand, T, Jaddoe, V, Hofman, A, Mackenbach, JP, Steegers, EA, et al. Physically Demanding Work, Fetal Growth and the Risk of Adverse Birth Outcomes. The Generation R Study. Occup Environ Med (2012) 69(8):543–50. doi:10.1136/oemed-2011-100615
45. Specht, IO, Hammer, PEC, Flachs, EM, Begtrup, LM, Larsen, AD, Hougaard, KS, et al. Night Work During Pregnancy and Preterm Birth-A Large Register-Based Cohort Study. PLoS One (2019) 14(4):e0215748. doi:10.1371/journal.pone.0215748
46. Vrijkotte, T, Brand, T, and Bonsel, G. First Trimester Employment, Working Conditions and Preterm Birth: A Prospective Population-Based Cohort Study. Occup Environ Med (2021) 78(9):654–60. doi:10.1136/oemed-2020-107072
47. Zhu, JL, Hjollund, NH, and Olsen, J, National Birth Cohort in Denmark. Shift Work, Duration of Pregnancy, and Birth Weight: The National Birth Cohort in Denmark. Am J Obstet Gynecol (2004) 191(1):285–91. doi:10.1016/j.ajog.2003.12.002
48. Bell, JF, Zimmerman, FJ, and Diehr, PK. Maternal Work and Birth Outcome Disparities. Matern Child Health J (2008) 12(4):415–26. doi:10.1007/s10995-007-0264-6
49. Lawson, CC, Whelan, EA, Hibert, EN, Grajewski, B, Spiegelman, D, and Rich-Edwards, JW. Occupational Factors and Risk of Preterm Birth in Nurses. Am J Obstet Gynecol (2009) 200(1):51 e1–8. doi:10.1016/j.ajog.2008.08.006
50. Lee, LJ, Symanski, E, Lupo, PJ, Tinker, SC, Razzaghi, H, Chan, W, et al. Role of Maternal Occupational Physical Activity and Psychosocial Stressors on Adverse Birth Outcomes. Occup Environ Med (2017) 74(3):192–9. doi:10.1136/oemed-2016-103715
51. Magann, EF, Evans, SF, Chauhan, SP, Nolan, TE, Henderson, J, Klausen, JH, et al. The Effects of Standing, Lifting and Noise Exposure on Preterm Birth, Growth Restriction, and Perinatal Death in Healthy Low-Risk Working Military Women. J Matern Fetal Neonatal Med (2005) 18(3):155–62. doi:10.1080/14767050500224810
52. Pompeii, LA, Savitz, DA, Evenson, KR, Rogers, B, and McMahon, M. Physical Exertion at Work and the Risk of Preterm Delivery and Small-For-Gestational-Age Birth. Obstet Gynecol (2005) 106(6):1279–88. doi:10.1097/01.AOG.0000189080.76998.f8
53. Stinson, JC, and Lee, KA. Premature Labor and Birth: Influence of Rank and Perception of Fatigue in Active Duty Military Women. Mil Med (2003) 168(5):385–90. doi:10.1093/milmed/168.5.385
54. von Ehrenstein, OS, Wilhelm, M, Wang, A, and Ritz, B. Preterm Birth and Prenatal Maternal Occupation: The Role of Hispanic Ethnicity and Nativity in a Population-Based Sample in Los Angeles, California. Am J Public Health (2014) 104(1):S65–72. doi:10.2105/AJPH.2013.301457
55. Celikkalp, U, and Yorulmaz, F. The Effect of Occupational Risk Factors on Pregnancy and Newborn Infants of Pregnant Midwives and Nurses in Turkey: A Prospective Study. Int J Caring Sci (2017) 10(2):690.
56. Takeuchi, M, Rahman, M, Ishiguro, A, and Nomura, K. Long Working Hours and Pregnancy Complications: Women Physicians Survey in Japan. BMC pregnancy and childbirth (2014) 14(1):245–8. doi:10.1186/1471-2393-14-245
57. Shirangi, A, Fritschi, L, and Holman, CDJ. Associations of Unscavenged Anesthetic Gases and Long Working Hours With Preterm Delivery in Female Veterinarians. Obstet Gynecol (2009) 113(5):1008–17. doi:10.1097/AOG.0b013e31819fe996
58. Croteau, A, Marcoux, S, and Brisson, C. Work Activity in Pregnancy, Preventive Measures, and the Risk of Preterm Delivery. Am J Epidemiol (2007) 166(8):951–65. doi:10.1093/aje/kwm171
59. Agbla, F, Ergin, A, and Boris, NW. Occupational Working Conditions as Risk Factors for Preterm Birth in Benin, West Africa. Rev Epidemiol Sante Publique (2006) 54(2):157–65. doi:10.1016/s0398-7620(06)76709-8
60. Arafa, MA, Amine, T, and Abdel Fattah, M. Association of Maternal Work With Adverse Perinatal Outcome. Can J Public Health (2007) 98:217–21. doi:10.1007/BF03403716
61. El-Gilany, A, El-Khawaga, G, and Ghanem, A. Incidence and Occupational Risk Factors of Preterm Delivery Among Working Mothers: A Single Center Study in Egypt. TAF Prev Med Bull (2016) 15(3):199. doi:10.5455/pmb.1-1441637597
62. Omokhodion, FO, Onadeko, MO, Roberts, OA, Beach, JR, Burstyn, I, and Cherry, NM. Paid Work, Domestic Work, and Other Determinants of Pregnancy Outcome in Ibadan, Southwest Nigeria. Int J Gynaecol Obstet (2010) 111(2):165–70. doi:10.1016/j.ijgo.2010.06.016
63. Abeysena, C, Jayawardana, P, and Seneviratne Rde, A. Effect of Psychosocial Stress and Physical Activity on Preterm Birth: A Cohort Study. J Obstet Gynaecol Res (2010) 36(2):260–7. doi:10.1111/j.1447-0756.2009.01160.x
64. Davari, MH, Naghshineh, E, Mostaghaci, M, Mirmohammadi, SJ, Bahaloo, M, Jafari, A, et al. Shift Work Effects and Pregnancy Outcome: A Historical Cohort Study. J Fam Reprod Health (2018) 12(2):84–8.
65. Nelson, K, Lohsoonthorn, V, and Williams, MA. Preterm Delivery Risk in Relation to Maternal Occupational and Leisure Time Physical Activity Among Thai Women. Asian Biomed Res Rev News (2009) 3(3):267–77.
66. Sumsrisuwan, N, Kongwattanakul, K, and Saksiriwuttho, P. Pregnancy Outcomes in Nurses and Nursing Assistants. Thai J Obstet Gynaecol (2015) 2015:89–95.
67. Manuck, TA, Rice, MM, Bailit, JL, Grobman, WA, Reddy, UM, Wapner, RJ, et al. Preterm Neonatal Morbidity and Mortality by Gestational Age: A Contemporary Cohort. Am J Obstet Gynecol (2016) 215(1):103.e1–103.e14. doi:10.1016/j.ajog.2016.01.004
68. Walani, SR. Global Burden of Preterm Birth. Int J Gynecol Obstet (2020) 150(1):31–3. doi:10.1002/ijgo.13195
69. Gamble, KL, Resuehr, D, and Johnson, CH. Shift Work and Circadian Dysregulation of Reproduction. Front Endocrinol (2013) 4:92. doi:10.3389/fendo.2013.00092
70. Boivin, DB, Boudreau, P, and Kosmadopoulos, A. Disturbance of the Circadian System in Shift Work and its Health Impact. J Biol rhythms (2022) 37(1):3–28. doi:10.1177/07487304211064218
71. James, SM, Honn, KA, Gaddameedhi, S, and Van Dongen, HP. Shift Work: Disrupted Circadian Rhythms and Sleep—Implications for Health and Well-Being. Curr Sleep Med Rep (2017) 3:104–12. doi:10.1007/s40675-017-0071-6
72. Simpson, JL. Are Physical Activity and Employment Related to Preterm Birth and Low Birth Weight? Am J Obstet Gynecol (1993) 168(4):1231–8. doi:10.1016/0002-9378(93)90374-r
73. Fernandez, CR, Betancur, JO, and de la Cuadra, JP. Athletic Body Stereotypes in the Academic Training of Students in the Physical Activity and Sport Sciences. J Hum Sport Exerc (2016) 11(1):74–88.
74. Nakamura, H, Ohsu, W, Nagase, H, Okazawa, T, Yoshida, M, and Okada, A. Uterine Circulatory Dysfunction Induced by Whole-Body Vibration and its Endocrine Pathogenesis in the Pregnant Rat. Eur J Appl Physiol Occup Physiol (1996) 72:292–6. doi:10.1007/BF00599687
75. Holzman, C, Senagore, P, Tian, Y, Bullen, B, DeVos, E, Leece, C, et al. Maternal Catecholamine Levels in Midpregnancy and Risk of Preterm Delivery. Am J Epidemiol (2009) 170(8):1014–24. doi:10.1093/aje/kwp218
76. Ferguson, KK, O'Neill, MS, and Meeker, JD. Environmental Contaminant Exposures and Preterm Birth: A Comprehensive Review. J Toxicol Environ Health B. (2013) 16(2):69–113. doi:10.1080/10937404.2013.775048
77. Gisselmann, MD, and Hemström, Ö. The Contribution of Maternal Working Conditions to Socio-Economic Inequalities in Birth Outcome. Soc Sci Med (2008) 66(6):1297–309. doi:10.1016/j.socscimed.2007.11.036
78. Guendelman, S, Pearl, M, Kosa, JL, Graham, S, Abrams, B, and Kharrazi, M. Association Between Preterm Delivery and Pre-Pregnancy Body Mass (BMI), Exercise and Sleep during Pregnancy Among Working Women in Southern California. Matern child Health J (2013) 17:723–31. doi:10.1007/s10995-012-1052-5
79. Mekonnen, ZK, Oehlert, JW, Eskenazi, B, Shaw, GM, Balmes, JR, and Padula, AM. The Relationship Between Air Pollutants and Maternal Socioeconomic Factors on Preterm Birth in California Urban Counties. J Expo Sci Environ Epidemiol (2021) 31(3):503–13. doi:10.1038/s41370-021-00323-7
80. Hämmig, O. Prevalence and Health Correlates of Work-Life Conflict Among Blue-And White-Collar Workers From Different Economic Sectors. Front Public Health (2014) 2:221. doi:10.3389/fpubh.2014.00221
81. Jayaram, A, Collier, CH, and Martin, JN. Preterm Parturition and Pre-eclampsia: The confluence of Two Great Gestational Syndromes. Int J Gynecol Obstet (2020) 150(1):10–6. doi:10.1002/ijgo.13173
82. Auger, N, Le, TUN, Park, AL, and Luo, Z-C. Association Between Maternal Comorbidity and Preterm Birth by Severity and Clinical Subtype: Retrospective Cohort Study. BMC pregnancy and childbirth (2011) 11(1):67–10. doi:10.1186/1471-2393-11-67
83. Haelterman, E, Marcoux, S, Croteau, A, and Dramaix, M. Population-Based Study on Occupational Risk Factors for Preeclampsia and Gestational Hypertension. Scand J work, Environ Health (2007) 33:304–17. doi:10.5271/sjweh.1147
85. WHO. Standards for Improving Quality of Maternal and Newborn Care in Health Facilities (2016). Available from: https://www.who.int/publications/i/item/9789241511216 (Accessed September 19, 2023).
86. Butterworth, P, Leach, LS, Strazdins, L, Olesen, SC, Rodgers, B, and Broom, DH. The Psychosocial Quality of Work Determines Whether Employment Has Benefits for Mental Health: Results From a Longitudinal National Household Panel Survey. Occup Environ Med (2011) 68(11):806–12. doi:10.1136/oem.2010.059030
Keywords: pregnancy, systematic review, meta-analysis, preterm birth, occupational risks
Citation: Adane HA, Iles R, Boyle JA, Gelaw A and Collie A (2023) Maternal Occupational Risk Factors and Preterm Birth: A Systematic Review and Meta-Analysis. Public Health Rev 44:1606085. doi: 10.3389/phrs.2023.1606085
Received: 14 April 2023; Accepted: 01 October 2023;
Published: 23 October 2023.
Edited by:
Gemma Castaño-Vinyals, Instituto Salud Global Barcelona (ISGlobal), SpainReviewed by:
Yayehirad Melsew, Monash University, AustraliaCopyright © 2023 Adane, Iles, Boyle, Gelaw and Collie. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
PHR is edited by the Swiss School of Public Health (SSPH+) in a partnership with the Association of Schools of Public Health of the European Region (ASPHER)+
*Correspondence: Haimanot Abebe Adane, aGFpbWFub3QuYWRhbmVAbW9uYXNoLmVkdQ==