 Gilbert T. Chua1†
Gilbert T. Chua1† Keith T. S. Tung1†
Keith T. S. Tung1† Mike Yat Wah Kwan2†
Mike Yat Wah Kwan2† Rosa S. Wong1Celine S. L. Chui1,3Xue Li3,4
Rosa S. Wong1Celine S. L. Chui1,3Xue Li3,4 Wilfred H. S. Wong1Winnie W. Y. Tso1King Wa Fu5
Wilfred H. S. Wong1Winnie W. Y. Tso1King Wa Fu5 Ko Ling Chan6
Ko Ling Chan6 Yun Kwok Wing7Eric Yu Hai Chen8,9
Yun Kwok Wing7Eric Yu Hai Chen8,9 Tatia Mei Chun Lee9
Tatia Mei Chun Lee9 Nirmala Rao10Godfrey C. F. Chan1
Nirmala Rao10Godfrey C. F. Chan1 Ellis K. L. Hon11Ivan Fan Ngai Hung4Kui Kai Lau4
Ellis K. L. Hon11Ivan Fan Ngai Hung4Kui Kai Lau4 Marco H. K. Ho1Kirstie Wong1Xiaoli Xiong12Shuiqing Chi13Shao-tao Tang13
Marco H. K. Ho1Kirstie Wong1Xiaoli Xiong12Shuiqing Chi13Shao-tao Tang13 Paul K. H. Tam14,15
Paul K. H. Tam14,15 Ian C. K. Wong3,16*
Ian C. K. Wong3,16* Patrick Ip1*
Patrick Ip1*- 1Department of Paediatrics and Adolescent Medicine, LKS Faculty of Medicine, The University of Hong Kong, Hong Kong SAR, China
- 2Department of Paediatrics and Adolescent Medicine, Princess Margaret Hospital, Hong Kong SAR, China
- 3Centre for Safe Medication Practice and Research, Department of Pharmacology and Pharmacy, The University of Hong Kong, Hong Kong SAR, China
- 4Department of Medicine, LKS Faculty of Medicine, The University of Hong Kong, Hong Kong SAR, China
- 5Journalism and Media Studies Centre, The University of Hong Kong, Hong Kong SAR, China
- 6Department of Applied Social Sciences, The Hong Kong Polytechnic University, Hong Kong SAR, China
- 7Department of Psychiatry, Faculty of Medicine, The Chinese University of Hong Kong, Hong Kong SAR, China
- 8Department of Psychiatry, LKS Faculty of Medicine, The University of Hong Kong, Hong Kong SAR, China
- 9State Key Laboratory of Brain and Cognitive Science, The University of Hong Kong, Hong Kong SAR, China
- 10Faculty of Education, The University of Hong Kong, Hong Kong SAR, China
- 11The Hong Kong Children’s Hospital, Hong Kong SAR, China
- 12Department of Integrated Chinese and Western Medicine, Wuhan Children’s Hospital (Wuhan Maternal and Child Healthcare Hospital), Tongji Medical College, Huazhong University of Science and Technology, Wuhan, China
- 13Department of Paediatric Surgery, Union Hospital, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, China
- 14Department of Surgery, LKS Faculty of Medicine, The University of Hong Kong, Hong Kong SAR, China
- 15Dr. Li Dak Sum Research Centre, The University of Hong Kong-Karolinska Institutet Collaboration in Regenerative Medicine, The University of Hong Kong, Hong Kong SAR, China
- 16Research Department of Practice and Policy, UCL School of Pharmacy, University College London, London, United Kingdom
Objectives: This study aimed to identify key factors affecting Healthcare workers (HCWs) perceived stress and risk of contracting COVID-19 among themselves and their family members during the pandemic.
Methods: A cross-sectional online questionnaire study was conducted between 19 March and April 5, 2020 in Hong Kong. HCWs from public hospitals and private dentists, and their family members participated.
Results: A total of 747 HCWs and 245 family members participated. Higher perceived stress in HCWs was associated with more negative changes in family relationship (p = 0.025). The HCWs’ perceived stress, however, was positively associated with family cohesion (p = 0.033) and stress levels of family members (p < 0.001). The level of HCWs’ satisfaction toward the hospital policies in response to the COVID-19 outbreak was associated with lower levels of perceived stress and risk of themselves or their family members contracting COVID-19. HCWs’ previous frontline experience of SARS was significantly associated with less perceived risk of themselves or their family members contracting COVID-19.
Conclusion: Hospital policies addressing HCWs’ needs, frontline experience of SARS, and family relationship influenced psychological wellbeing of HCWs during the COVID-19 outbreak.
Introduction
The coronavirus disease 2019 (COVID-19) pandemic due to severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) has already caused more than 34 million confirmed cases and over one million deaths worldwide as of early-October 2020 [1]. Healthcare workers (HCWs) have a very high risk of being infected by SARS-CoV-2 and are increasingly worried about potentially infecting their family members [2, 3]. This situation is worsen by the chronic shortage of personal protective equipment (PPE) worldwide [4]. Recent reports have revealed that exposure to SARS-CoV-2 while caring for patients due to lack of PPE has led to many HCWs becoming infected by COVID-19 and many have sadly died. The unfamiliarity and perceived uncontrollability of the COVID-19 might hamper the psychological wellbeing of the HCWs.
Previous evidence already suggest that HCWs are susceptible to psychological distress, anxiety, post-traumatic stress disorder, sleep disturbances, and burnout during and after major infectious disease outbreaks [5–7]. Risk factors affecting their wellbeing include beliefs about their increased likelihood of infection, heightened concern of infecting their family members, increased workload, stress, lack of available precautionary measures, nature of their work, and family structures [8–10]. During the SARS outbreak, HCWs in Hong Kong who survived from SARS infection were 2.24 times more likely to develop psychiatric morbidities than non-HCW survivors, which lasted up to 3.5 years after the end of the epidemic [11]. In the COVID-19 pandemic, HCWs in China reported high levels of anxiety, and stress, and low self-efficacy, with associated poor sleep quality and weak social support [12]. However, only a few studies focused on the risk and protective factors contributing to HCWs’ psychological wellbeing. Understanding the contributing factors to HCWs’ psychological wellbeing would provide insightful advice on how to mitigate the escalating stress level of HCWs during infectious diseases outbreak. An investigation of the psychological wellbeing of HCWs during the COVID-19 outbreak and the factors affecting their mental health is urgently warranted.
This study aimed to examine the levels of HCWs’ perceived stress and risk of infection by COVID-19 while caring for patients during the pandemic and to identify how individual, family, and policy factors, and previous frontline experience during the SARS 2003 outbreak influenced these outcomes.
Methods
Study Participants
This was a cross-sectional online questionnaire study of HCWs and their family members at the peak of the COVID-19 pandemic in Hong Kong. The inclusion criteria for participation in the study included HCWs working in the Hong Kong public healthcare system such as doctors, dentists, nurses, allied health professionals, pharmacists, and healthcare assistants; dentists working in the private sector; and both HCWs and their family members aged 18 years or above. We disseminated the online survey through the public hospital network and the web-link was published on several websites affiliated with key HCW associations in Hong Kong. After providing consent electronically, recruited subjects (HCWs and their family members) were invited to complete the questionnaire, which was available in both English (Supplementary Material) and Chinese. We linked the responses of HCWs and their family members using a unique identification number.
Measurements
The study questionnaires covered basic characteristics, mental health status, family relationships, and risk perception of HCWs and family members contracting COVID-19.
Demographics
We obtained detailed information from HCWs regarding the nature of their job, experience of managing suspected or confirmed COVID-19 cases and cohabitation status, as well as previous frontline experience of the SARS 2003 outbreak.
Perceived Stress
Both HCWs and their family members were asked to rate their perceived stress level respectively using the 10-item Perceived Stress Scale (PSS-10), which is a widely used instrument for measuring psychological distress that has been validated in the Chinese population [13]. The 10 items are scored on a 5-point scale from 0 to 4 and the total score is out of 40. A higher score indicated higher level of perceived stress.
Perceived Family Cohesion and Changes in Family Relationships
Both HCWs and their family members were asked to rate separately their perceived family support using the Family APGAR (Adaption, Partnership, Growth, Affection, Resolve) scale, which has been validated in the Chinese population [14]. This scale has five items rated on a 3-point scale and a total score out of 15. A higher total score indicated better perceived family cohesion. They were also asked to rate the perceived change in family relationship during the COVID-19 outbreak.
Risk Perception
The HCWs were asked “How bad do you feel if you were diagnosed with COVID-19” and to rate their perceived risk of infection by COVID-19 on a 5-point scale from “not bad at all” to “very bad.” This reflected how badly they would feel if they or their family members were diagnosed with COVID-19. A higher score indicated a higher perceived risk of infection.
Satisfaction Toward Hospital Policies in Response to the COVID-19 Outbreak
The HCWs were asked to rate their satisfaction toward hospital policies in response to the COVID-19 outbreak, which included the provision of PPE for those working in high-risk areas (e.g., isolation wards), PPE for those working in non-high-risk areas (e.g., outpatient clinics), special accommodation allowance for HCWs working in high-risk areas to stay at hotels to prevent transmitting COVID-19 to family members, and special salary increments for HCWs working in high-risk areas. The four items were rated on a 5-point scale between −2 and +2, and the total score represented the overall satisfaction. As most dentists in Hong Kong work in the private sector, their responses were excluded from this analysis.
Data Analysis
We used Student’s t-test, Chi-square test and Fisher’s exact test to compare the perceived stress and risk of being diagnosed with COVID-19 across different groups as appropriate. The relationships between the study variables were examined using bivariate correlations. A series of regression models were conducted to explore the factors associated with HCWs’ perceived levels of stress and risk of infection during the COVID-19 outbreak. Univariate regression analyses were first conducted to measure the crude independent effects of different factors including age, role in healthcare sector, perceived level of family cohesion and changes in family relationships during COVID-19 outbreak, satisfaction toward the overall and individual hospital special policies, and measures of HCWs, and perceived stress levels and family relationships of family members. Multiple regression models were performed to examine the adjusted associations while controlling for the impacts of sex, marital status, role in healthcare sector, age, and number of years of work experience. All statistical analyses were conducted using SPSS version 25.0 (IBM, Armonk, New York, United States). All statistical tests were two-tailed and a p-value of less than 0.05 was considered statistically significant.
Result
Between 19 March and April 5, 2020, a total of 747 HCWs and 245 family members completed the online questionnaires. Table 1 summarizes the demographics of HCWs who participated in this study and the overall responses. The mean age of HCWs was 39.6 years (SD = 10.9), 27% were male, and over 60% were married or cohabitating. The average years of work experience was 13 years (SD = 7.7). The majority of HCWs were nurses (45.7%) and doctors (23.0%). Approximately 20% (149/747) of the respondents worked in COVID-19 high-risk areas and 10.4% (78/747) had direct contact with confirmed COVID-19 patients. Over 90% of HCWs experienced the SARS outbreak in Hong Kong, with 44.2% working in the healthcare sector during the SARS outbreak. About 15% of HCWs reported they had a peer, colleague, or family member that had been infected or died due to SARS. The mean stress levels of HCWs and their family members were 21.3 and 21.1, respectively. Family cohesion scores of HCWs and their family members were 11.8 and 12.0 respectively. Family relationships during the COVID-19 outbreak were reported to be improved in 23.0% of HCWs, but deteriorated in 10.04%, whereas 66.8% reported to have no changes. Overall, HCWs reported dissatisfaction of hospital support in response to the COVID-19 outbreak.
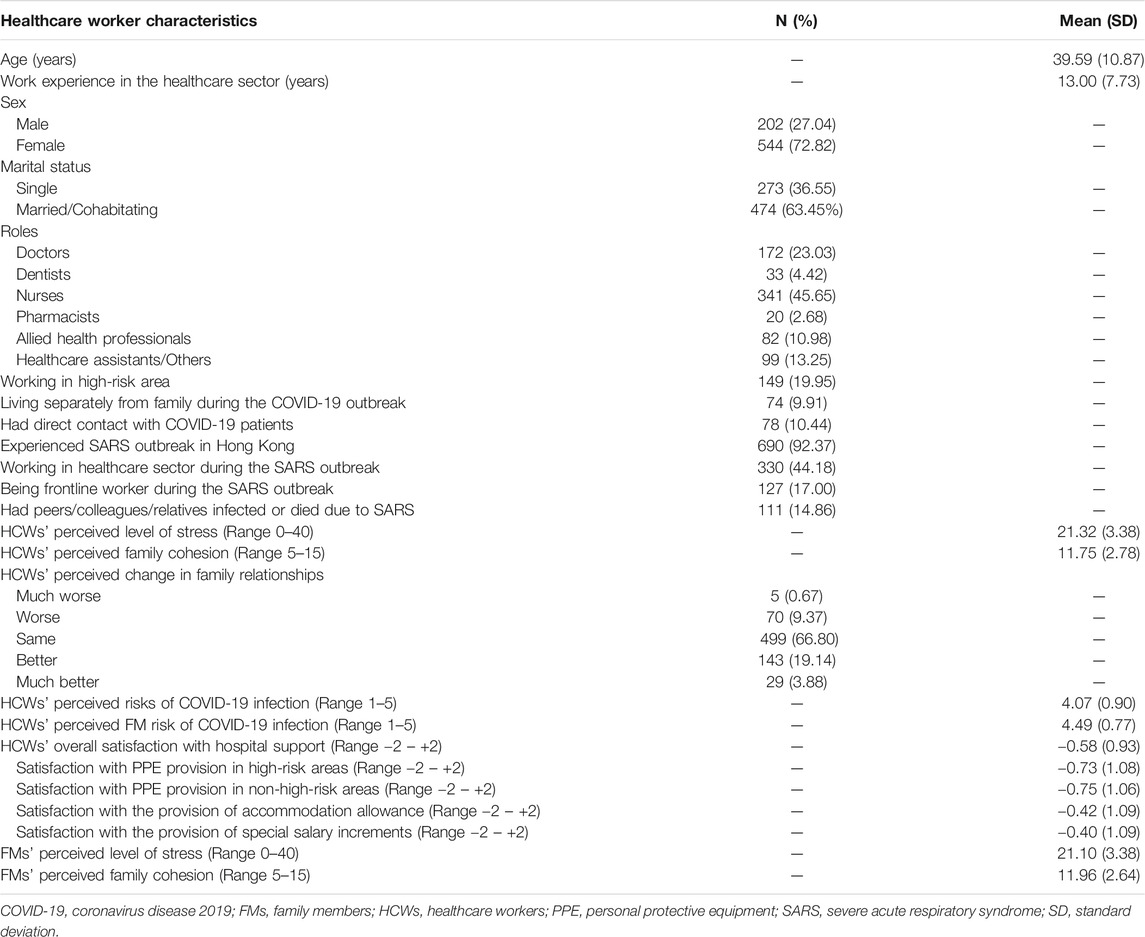
TABLE 1. Healthcare worker demographics and overall responses in Hong Kong between 19 March and April 5, 2020.
Table 2 describes mean levels of perceived stress and risk of COVID-19 infection of HCWs and their family members by participants’ characteristics. Between-group comparisons showed that HCWs in different roles had significantly different mean stress scores and mean risk scores for COVID-19 infection for themselves and their family members (all p < 0.05). The HCWs who worked in the healthcare sector and those on the frontline caring for SARS patients had significantly lower perceived risk of COVID-19 infection for themselves and their family members (all p < 0.05). However, HCWs working in high-risk areas and their decision to live separately from their families was not correlated with their perceived levels of stress and risk of COVID-19 infection.
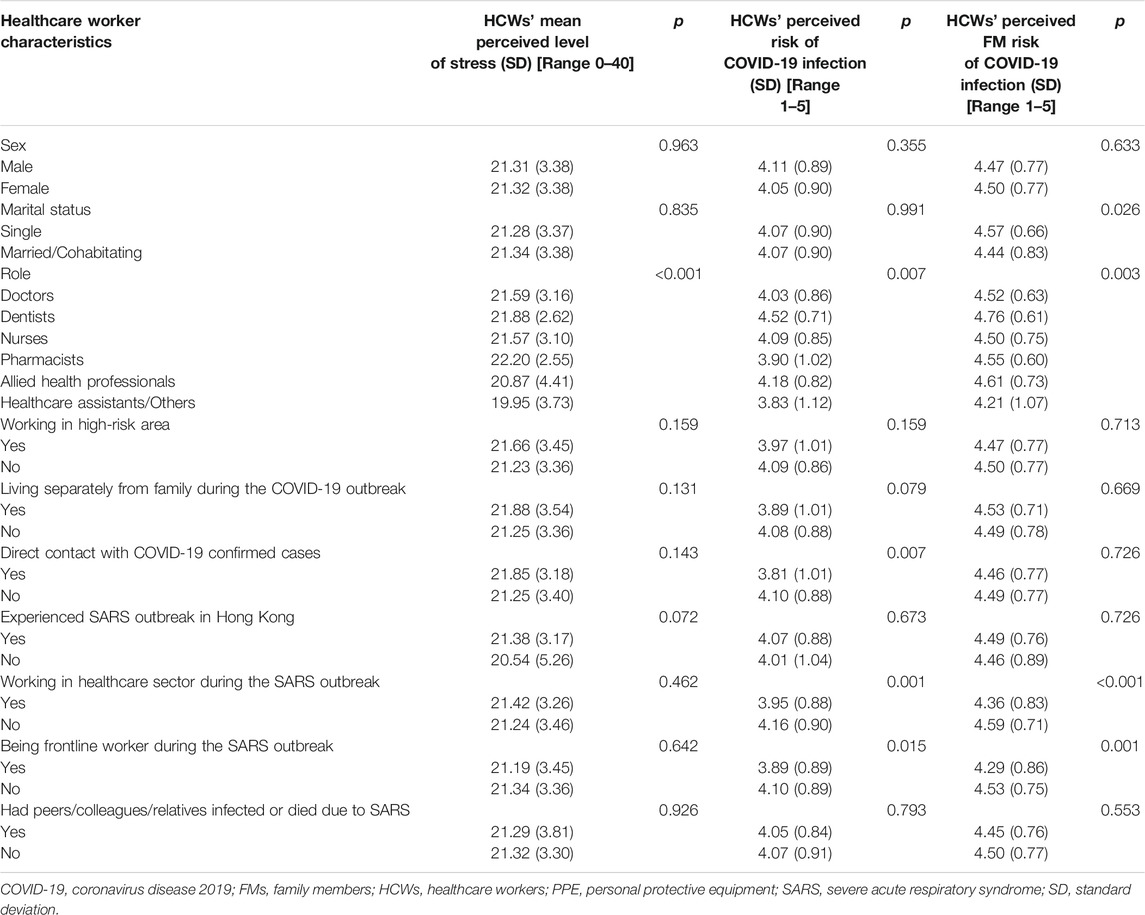
TABLE 2. Healthcare workers’ perceived levels of stress and risk of contracting COVID-19 in Hong Kong between 19 March and April 5, 2020.
Correlation analyses (Table 3) demonstrated the HCWs’ perceived stress was positively associated with their perceived risk of COVID-19 infection (r = 0.218), family members’ risk of COVID-19 infection (r = 0.199), and family members’ stress levels (r = 0.237) (all p < 0.001). Whereas, both HCWs’ perceived risk of COVID-19 infection for themselves and their family members were negatively correlated with their satisfaction with hospital policies (r = −0.219–−0.278, p < 0.001). Age and years of work experience were also negatively correlated with their perceived risk of COVID-19 infection for themselves and their family members.
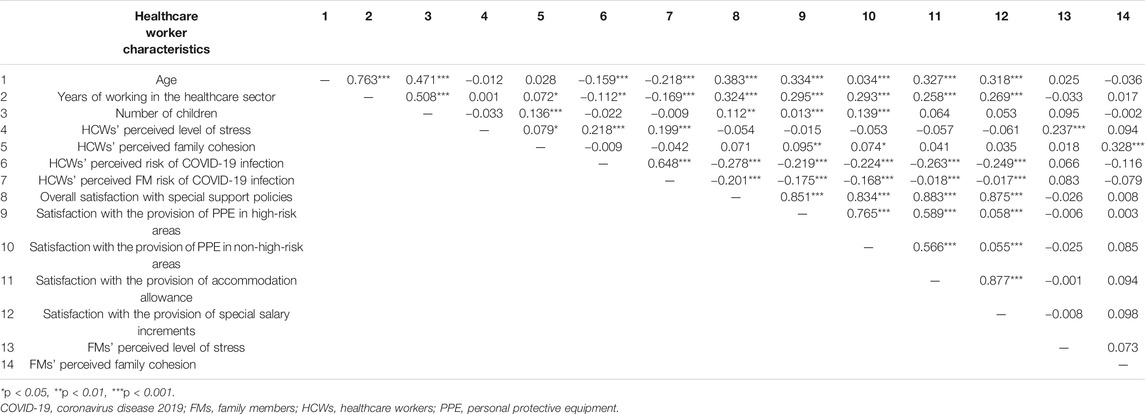
TABLE 3. Pearson correlation matrix for continuous variables between the characteristics of healthcare workers in Hong Kong between 19 March and April 5, 2020.
Table 4 displays the adjusted association of different factors with the HCWs’ perceived levels of stress and risk of COVID-19 infection for themselves and their family members. Doctors nurses and dentists were found to have significantly higher level of stress compared to allied health professionals, healthcare assistants, and others (p = 0.001). Higher perceived stress in HCWs was associated with more negative changes in family relationship (p = 0.025). The HCWs’ perceived stress level was also positively associated with their perceived family cohesion (p = 0.033), and stress levels of family members (p < 0.001). The HCWs’ satisfaction with overall and individual special hospital policies in response to the COVID-19 outbreak were negatively associated with their perceived levels of stress (all p < 0.05, except PPE provision in high-risk areas), and risk of contracting COVID-19 for themselves and their family members (all p < 0.001). HCWs with experience of working in healthcare sector or with frontline experience during SARS outbreak were found to have significantly lower perceived risk of COVID-19 infection for themselves and their family members (all p < 0.01).
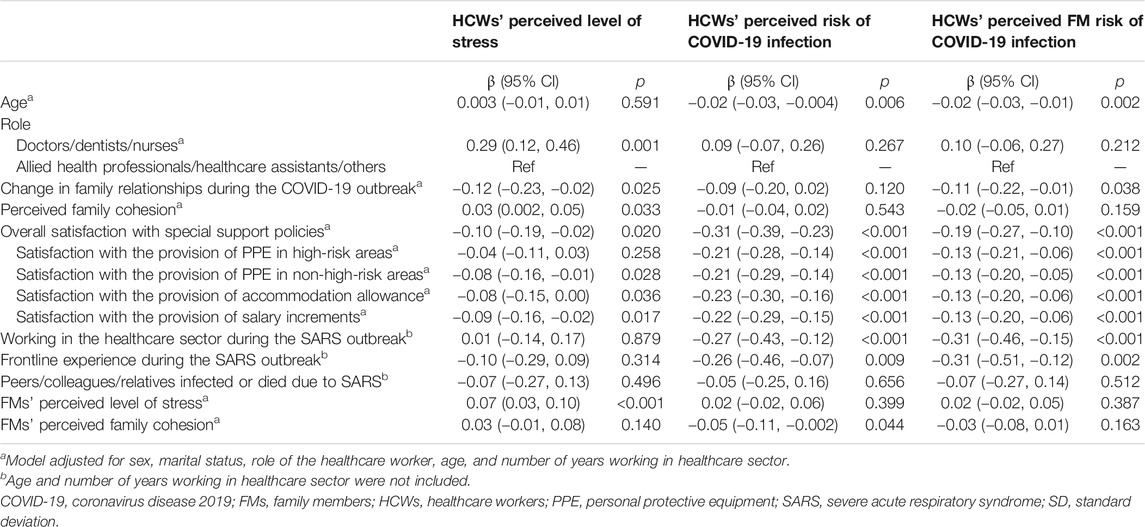
TABLE 4. Adjusted associations between individual, family, and policy factors with outcomes of healthcare workers in Hong Kong between 19 March and April 5, 2020.
Discussion
This study was conducted at the peak of the COVID-19 outbreak in Hong Kong [15]. To the best of our knowledge, this study is one of the first to examine HCWs’ perceived levels of stress and their perceived risk of contracting COVID-19 for themselves and their family members when the government is undertaking a set of measures to protect citizens and communities. This is also the first study to examine how previous frontline experience of the SARS outbreak and family factors are associated with HCWs’ psychological wellbeing during the pandemic.
The SARS epidemic in Hong Kong is unique as not all regions of the world were severely affected by the SARS outbreak. Our study showed that the experience as frontline workers during the SARS outbreak was associated with a lower perceived risk of contracting COVID-19 for the HCWs and their family members after adjusting for sex, marital status, and role. Age and years of experience were not included in the adjusted model, as all HCWs who had experienced the SARS epidemic were senior staff. Such observation is possibly explained by the fact that SARS-CoV and SARS-CoV-2 shared similarities in terms of their genomic sequences and biology [16]. This may also signifies that experience in the COVID-19 pandemic could benefit HCWs in facing infectious disease outbreaks in the future.
The mean stress scores in this study indicated a moderate level of stress among the HCWs and their family members in fighting COVID-19, which was similar to other parts of the world, including China, Singapore, North America, the Middle East and Europe [17–21]. The perceived levels of stress in HCWs were significantly and negatively associated with changes in family relationships over the COVID-19 outbreak period. Family support has been proposed to mitigate psychological distress experienced by HCWs particularly in the face of the overwhelming burden of COVID-19 onto the healthcare system [22]. Another stressor for HCWs was the stress and anxiety experienced by their family members during the outbreak. It is inevitable that laypersons would also suffer from mental health disturbances in this pandemic. This is not only because of the fear of contracting the diseases but also due to a dramatic change in lifestyles, social and political atmospheres and economical impact [23, 24]. It is possible that the vicious circle of stressful responses between HCWs and their family members might worsen the health and wellbeing of each other. We also observed a positive correlation between HCWs’ perceived risk of contracting COVID-19 for themselves and their family members, suggesting the possibility of higher apprehension in the HCWs due to the perception of their own infection risk and also their family members’ risk of getting infected. In addition, concerns about the health of the family and fear of spreading the infection to family members can be other sources of stress [9, 25, 26]. In Canada and the United States, many HCWs have opted to live separately from their family, such as paying to stay at a hotel or in donated recreational vehicles [27, 28]. Our study demonstrated that satisfaction toward allowances for accommodation could considerably alleviate HCWs’ stress and their perceived risk of infecting family members. The Hong Kong Hospital Authority implemented a special salary increment and rental allowance scheme, and liaized with local hotels to support HCWs to isolate themselves from their families while working in high-risk areas [29, 30]. We found that 55.4% of HCWs who had been in direct contact with COVID-19 patients also opted to live away from their family during the COVID-19 outbreak, indicating that accommodation support is needed in a pandemic. This concurs with a recent study in Saudi Arabia that living with co-habitants predicted higher level of concerns among HCWs [21].
Our study demonstrated that HCWs’ perceived level of stress was significantly associated with their job role. Doctors, nurses, and dentists who were frequently in contact with infected patients experienced higher levels of stress than other supporting staff. Standard precautions including barrier protection, such as masks, face-shields, and disposal gowns, are recommended to protect them from airborne infections, and was proven to be effective in Hong Kong where no HCWs were being infected with COVID-19 in their workplace [31–33]. This was supported by our study results that satisfaction with hospital’s provision of PPE can significantly reduce HCWs’ perceived level of stress and risk of contracting COVID-19 for themselves and their family members. However, the global shortage of PPE and the lack of government support may have aggravated the perceived risk of infection of HCWs during the COVID-19 outbreak. It has been reported that some HCWs threatened to stop working due to the lack of PPE [34]. These reports further highlight the profound impacts of worldwide PPE shortage during the COVID-19 pandemic on the psychological wellbeing of HCWs. To overcome the challenges, the Hong Kong government has implemented the policy of stockpiling PPE to protect the health and wellbeing of our frontline healthcare workers during the infectious disease outbreaks. During the SARS outbreak, a high number of HCWs who worked in intensive care units were infected from exposure to high-risk procedures, including the use of nebulizers, endotracheal suction, and intubation [35, 36]. These SARS experiences have led the Hong Kong government to regularly update and improve guidelines for frontline staff in the triage of suspected cases and in implementing protective measures for HCWs [37]. For example, after the SARS epidemic, ward facilities in Hong Kong underwent substantial improvements with modified protocols for those with suspected infectious diseases. Contingency plans were established to ensure 3-months stocks of PPE and the availability of portable high-efficiency particulate air filters in clinical areas where permanent installation is not feasible [38]. These special preventive measures adopted in Hong Kong might serve as a good example to alleviate the psychological impacts on HCWs during infectious diseases outbreak. Concurring with a recent study in Hong Kong surveying more than 1,000 non-HCW, it demonstrated that workplace infection control policies and employees’ perception of infection risk directly impact on employees’ health outcomes, which the latter partly mediated the relationship between workplace infection control policies their health outcomes [39].
Recent studies have now focused on intervention to alleviate the adverse psychological impact of the COVID-19 pandemic on HCWs. In the United States, a multidisciplinary peer support model known as “Battle Buddies” was developed for the management of psychological stress exposure in providers deployed to disasters [40]. In China, the National Health Commission implemented policies with the joint effort of psychiatrists and mental health experts to handle emergency psychological crisis as a result of the COVID-19 outbreak. This policy targets specifically six high risks populations, including HCW, confirmed patients, their close contacts and other susceptible persons in the general public [41]. Digital platforms were also utilized in the United Kingdom to provide evidence-based support HCWs and their peers and families related to their psychological wellbeing [42]. As new waves of COVID-19 outbreaks was being anticipated in the coming winter, ongoing research in monitoring as well as the provision of timely intervention to mitigate the psychosocial wellbeing of HCWs and their families around the world will be needed.
This study had several limitations. First, this cross-sectional survey was carried out in Hong Kong during an outbreak period and did not measure the HCWs’ levels of stress and mental health status during the pre-outbreak period as comparison baseline levels. Second, the level of psychological distress in HCWs may change and hence this cross-sectional survey may not capture the fluctuations in stress levels over the highly dynamic course of the pandemic. Nevertheless, the study was conducted in the peak period of the COVID-19 outbreak [15] which was considered as the most stressful period of the pandemic and thus it should involve minimal recall bias. Third, the survey was distributed through healthcare worker networks and associations, which might be prone to potential sampling and volunteer bias. Respondents of our survey represented 2.7% of all doctors and 1.2% of all nurses employed by the Hong Kong Hospital Authority. Our respondents involved HCWs working in both high-risk and non-high risks areas, with a wide spectrum of working experiences (mean 13 years, SD 7.73). The mean age of our respondents was approximately 40 years old, which is close to the mean age of doctors, nurses and allied health professionals working in the Hospital Authority. Majority of our respondents were nurses and 72.8% of our respondents were females, which is similar to the nurse gender ratio working in the Hospital Authority. Therefore, respondents of our survey can be considered a representative sample.
Our study highlighted the key factors at the individual, family, and policy level affecting HCWs’ perceived level of stress and risk of being infected by COVID-19 for themselves and their family members during a pandemic. These factors included the nature of their work, change in family relationship during the outbreak, hospital policies, and prior experience of the SARS outbreak. Provision of adequate PPE and special allowance to the HCWs show great promise in protecting the psychological wellbeing of HCWs in fighting a pandemic.
Data Availability Statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics Statement
The studies involving human participants were reviewed and approved by the Institutional Review Board of the University of Hong Kong/Hospital Authority Hong Kong West Cluster (Reference Number UW 20-214). The patients/participants provided their written informed consent to participate in this study.
Author Contributions
GC, KT and MK contributed equally as co-first authors in conceptualizing, administrating, investigating, validating, writing and editing the manuscript. KT and RW led the analysis of the data. CC, XL, WW performed the analysis. PI and IW, as co-corresponding authors, conceptualized and supervised the project, administrated the questionnaires, validated the data, wrote and edited the manuscript. All authors contributed equally in conceptualizing and supervising the project, administering the questionnaires, validating and analyzing data, and editing the manuscript. All authors have approved the final manuscript as submitted.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.ssph-journal.org/articles/10.3389/ijph.2021.599408/full#supplementary-material.
References
1.World Health Organization. Coronavirus disease (COVID-19) situation report – 147. Geneva, Switzerland: World Health Organization (2020).
2.The Lancet. COVID-19: protecting health-care workers. Lancet (2020). :395(10228):922. doi:10.1016/S0140-6736(20)30644-9
3.BBC News. Coronavirus: remembering the NHS workers who have died. (2020). Available at: https://www.bbc.com/news/health-52242856. (Accessed April 20, 2020).
4.World Health Organization. Shortage of personal protective equipment endangering health workers worldwide. (2020). Available at: https://www.who.int/news-room/detail/03-03-2020-shortage-of-personal-protective-equipment-endangering-health-workers-worldwide. (Accessed April 20, 2020).
5. McAlonan, GM, Lee, AM, Cheung, V, Cheung, C, Tsang, KW, Sham, PC, et al. Immediate and sustained psychological impact of an emerging infectious disease outbreak on health care workers. Can J Psychiatry (2007). 52(4):241–7. doi:10.1177/070674370705200406
6. Su, TP, Lien, TC, Yang, CY, Su, YL, Wang, JH, Tsai, SL, et al. Prevalence of psychiatric morbidity and psychological adaptation of the nurses in a structured SARS caring unit during outbreak: a prospective and periodic assessment study in Taiwan. J Psychiatr Res (2007). 41(1-2):119–30. doi:10.1016/j.jpsychires.2005.12.006
7. Tam, CW, Pang, EP, Lam, LC, and Chiu, HF. Severe acute respiratory syndrome (SARS) in Hong Kong in 2003: stress and psychological impact among frontline healthcare workers. Psychol Med (2004). 34(7):1197–204. doi:10.1017/s0033291704002247
8. McMullan, C, Brown, GD, and O'Sullivan, D. Preparing to respond: Irish nurses’ perceptions of preparedness for an influenza pandemic. Int Emerg Nurs (2016). 26:3–7. doi:10.1016/j.ienj.2015.10.004
9. Nickell, LA, Crighton, EJ, Tracy, CS, Al-Enazy, H, Bolaji, Y, Hanjrah, S, et al. Psychosocial effects of SARS on hospital staff: survey of a large tertiary care institution. CMAJ (2004). 170(5):793–8. doi:10.1503/cmaj.1031077
10. Lin, CY, Peng, YC, Wu, YH, Chang, J, Chan, CH, and Yang, DY. The psychological effect of severe acute respiratory syndrome on emergency department staff. Emerg Med J (2007). 24(1):12–7. doi:10.1136/emj.2006.035089
11. Lam, MH, Wing, YK, Yu, MW, Leung, CM, Ma, RC, Kong, AP, et al. Mental morbidities and chronic fatigue in severe acute respiratory syndrome survivors: long-term follow-up. Arch Intern Med (2009). 169(22):2142–7. doi:10.1001/archinternmed.2009.384
12. Xiao, H, Zhang, Y, Kong, D, Li, S, and Yang, N. Social capital and sleep quality in individuals who self-isolated for 14 Days during the coronavirus disease 2019 (COVID-19) outbreak in january 2020 in China. Med Sci Monit (2020). 26:e923549. doi:10.12659/msm.923921
13. Wong, ATY, Chen, H, Liu, SH, Hsu, EK, Luk, KS, Lai, CKC, et al. From SARS to avian influenza preparedness in Hong Kong. Clin Infect Dis (2017). 64(Suppl_2):S98–s104. doi:10.1093/cid/cix123
14. Guo, N, Wang, MP, Luk, TT, Ho, SY, Fong, DYT, Chan, SS, et al. The association of problematic smartphone use with family well-being mediated by family communication in Chinese adults: a population-based study. J Behav Addict (2019). 8(3):412–9. doi:10.1556/2006.8.2019.39
15. Leung, GM, Cowling, BJ, and Wu, JT. From a sprint to a marathon in Hong Kong. N Engl J Med (2020). 382, e45. doi:10.1056/NEJMc2009790
16. Petrosillo, N, Viceconte, G, Ergonul, O, Ippolito, G, and Petersen, E. COVID-19, SARS and MERS: are they closely related? Clin Microbiol Infect (2020). 26, 729. doi:10.1016/j.cmi.2020.03.026
17. Tan, BYQ, Chew, NWS, Lee, GKH, Jing, M, Goh, Y, Yeo, LLL, et al. Psychological impact of the COVID-19 pandemic on health care workers in Singapore. Ann Intern Med (2020). 173(4):317–20. doi:10.7326/M20-1083
18. Stelnicki, AM, Carleton, RN, and Reichert, C. Nurses’ mental health and well-being: COVID-19 impacts. Can J Nurs Res (2020). 52(3):237–9. doi:10.1177/0844562120931623
19. Lai, J, Ma, S, Wang, Y, Cai, Z, Hu, J, Wei, N, et al. Factors associated with mental health outcomes among health care workers exposed to coronavirus disease 2019. JAMA Netw Open (2020). 3(3):e203976. doi:10.1001/jamanetworkopen.2020.3976
20. Franza, F, Basta, R, Pellegrino, F, Solomita, B, and Fasano, V. The role of fatigue of compassion, burnout and hopelessness in healthcare: experience in the time of COVID-19 outbreak. Psychiatr Danub (2020). 32(Suppl. 1):10–4.
21. Abolfotouh, MA, Almutairi, AF, BaniMustafa, AA, and Hussein, MA. Perception and attitude of healthcare workers in Saudi Arabia with regard to Covid-19 pandemic and potential associated predictors. BMC Infect Dis (2020). 20(1):719. doi:10.1186/s12879-020-05443-3
22. Lim, J, Bogossian, F, and Ahern, K. Stress and coping in Australian nurses: a systematic review. Int Nurs Rev (2010). 57(1):22–31. doi:10.1111/j.1466-7657.2009.00765.x
23. Pfefferbaum, B, and North, CS. Mental health and the covid-19 pandemic. N Engl J Med (2020). 383(6):510–2. doi:10.1056/NEJMp2008017
24. Mukhtar, S. Psychological health during the coronavirus disease 2019 pandemic outbreak. Int J Soc Psychiatry (2020). 66(5):512–6. doi:10.1177/0020764020925835
25. Maunder, R. The experience of the 2003 SARS outbreak as a traumatic stress among frontline healthcare workers in Toronto: lessons learned. Philos Trans R Soc Lond B Biol Sci (2004). 359(1447):1117–25. doi:10.1098/rstb.2004.1483
26. Harry, E. Stress and the healthcare worker. As complicated or as simple as fear and hope. J Med Pract Manage (2014). 30(1):28.
27.The Guardian. US medical workers self-isolate amid fears of bringing coronavirus home (2020). Available at: https://www.theguardian.com/world/2020/mar/19/medical-workers-self-isolate-home-fears-coronavirus (Accessed April 20, 2020).
28.USA Today. Families of health care workers are terrified they'll catch COVID-19 (2020). Available at: https://www.usatoday.com/story/news/nation/2020/03/28/coronavirus-rv-donations-doctors-nurses/2932617001/ (Accessed May 27, 2020).
29.Hong Kong Legislative Council. Measures for the prevention and control of coronavirus disease in Hong Kong (2020). Available at: https://www.legco.gov.hk/yr19-20/english/panels/hs/papers/hs20200310cb2-673-2-e.pdf (Accessed April 14, 2020).
30.Public hospitals mobilise resources. The Government of HKSAR (2020). Available at: https://www.news.gov.hk/eng/2020/01/20200124/20200124_143217_066.html (Accessed April 18, 2020).
31. Harrel, SK, and Molinari, J. Aerosols and splatter in dentistry: a brief review of the literature and infection control implications. J Am Dent Assoc (2004). 135(4):429–37. doi:10.14219/jada.archive.2004.0207
32. Lu, X, Zhang, L, Du, H, Zhang, J, Li, YY, Qu, J, et al. SARS-CoV-2 infection in children. N Engl J Med (2020). 382, 1663. doi:10.1056/NEJMc2005073
33. To, KKW, and Yuen, KY. Responding to COVID-19 in Hong Kong. Hong Kong Med J (2020). 26(3):164–6. doi:10.12809/hkmj205101
34. Davies, H. Advice on protective gear for NHS staff was rejected owing to cost (2020). Available at: https://www.theguardian.com/world/2020/mar/27/advice-on-protective-gear-for-nhs-staff-was-rejected-owing-to-cost (Accessed April 14, 2020).
35. Hung, LS. The SARS epidemic in Hong Kong: what lessons have we learned? J R Soc Med (2003). 96(8):374–8. doi:10.1258/jrsm.96.8.374
36. Tomlinson, B, and Cockram, C. SARS: experience at prince of wales hospital, Hong Kong. Lancet (2003). 361(9368):1486–7. doi:10.1016/s0140-6736(03)13218-7
37.Centre For Health Protection. Key elements on prevention and control of coronavirus disease (COVID-19) in healthcare settings. (2020). Available at: https://www.chp.gov.hk/files/pdf/ic_advice_for_nid_in_healthcare_setting.pdf (Accessed April 18, 2020).
38.Hospital Authority. HA contingency plan for SARS outbreak 2007 (2007). Available at: https://www.ha.org.hk/haho/ho/adm/131657e.pdf (Accessed April 22, 2020).
39. Wong, EL-Y, Ho, K-F, Wong, SY-S, Cheung, AW-L, Yau, PS-Y, Dong, D, et al. Views on workplace policies and its impact on health-related quality of life during coronavirus disease (COVID-19) pandemic: cross-sectional survey of employees. Int J Health Pol Manag (2020). doi:10.34172/ijhpm.2020.127
40. Albott, CS, Wozniak, JR, McGlinch, BP, Wall, MH, Gold, BS, and Vinogradov, S. Battle Buddies: rapid deployment of a psychological resilience intervention for health care workers during the COVID-19 pandemic. Anesth Analg (2020). 131(1):43–54. doi:10.1213/ane.0000000000004912
41. Dong, L, and Bouey, J. Public mental health crisis during COVID-19 pandemic, China. Emerg Infect Dis (2020). 26(7):1616–8. doi:10.3201/eid2607.200407
Keywords: COVID-19, healthcare workers, perceived stress, psychological wellbeing, hospital policies
Citation: Chua GT, Tung KTS, Kwan MYW, Wong RS, Chui CSL, Li X, Wong WHS, Tso WWY, Fu KW, Chan KL, Wing YK, Chen EYH, Chun Lee TM, Rao N, Chan GCF, Hon EKL, Hung IFN, Lau KK, Ho MHK, Wong K, Xiong X, Chi S, Tang S-t, Tam PKH, Wong ICK and Ip P (2021) Multilevel Factors Affecting Healthcare Workers’ Perceived Stress and Risk of Infection During COVID-19 Pandemic. Int J Public Health 66:599408. doi: 10.3389/ijph.2021.599408
Received: 27 August 2020; Accepted: 22 January 2021;
Published: 05 March 2021.
Edited by:
Calogero Guccio, University of Catania, ItalyCopyright © 2021 Chua, Tung, Kwan, Wong, Chui, Li, Wong, Tso, Fu, Chan, Wing, Chen, Chun Lee, Rao, Chan, Hon, Hung, Lau, Ho, Wong, Xiong, Chi, Tang, Tam, Wong and Ip. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Ian C. K. Wong, d29uZ2lja0Boa3UuaGs=; aS53b25nQHVjbC5hYy51aw==; Patrick Ip, cGF0cmljaXBAaGt1Lmhr