Abstract
Objectives: COVID-19 sanitary measures (social distancing, school closures) have deeply impacted social life, support networks, and their protective role in mental health. The present study aims to understand how attachment styles influence the way individuals experience social support. Particularly, investigating its moderating role in the relationship between social support and depression.
Methods: An online survey was designed to clarify the role of adult attachment styles (ECR-S) in the perceived social support (MOSS) and self-reported depressive symptoms (BDI-SF) in the COVID-19 context.
Results: Positive social interactions was the most important dimension of social support for lower depression symptoms. Individuals attachment strategies have a moderating role in the relation between of social support and depression. Crucially, insecure attachment style wanes the positive impact of social support in depression.
Conclusion: Aligned with the existing literature, attachment security is an essential factor in our current understanding of relationships and mental health. Exploring specific and indivual attachment strategies might be a powerful tool to protect population’s mental healt.
Introduction
Humans are primarily dependent on others for survival. This necessity underpins a set of behaviours to reach proximity with significant others (i.e., attachment strategies, [1]). The way in which our early social environment answered our needs is thought to be related to how we look for help later in our life, as well as how helpful we experience other’s support to be [2, 3]. These patterns would shape the social world in which our mental health is rooted [4–6].
From a health science perspective the resources that flow through and from social relationships are known as social support: the available support for individuals through social ties with other people, groups, or the community in general [7, 8].
Research and practice on mental health have been increasingly interested in social support, as it promotes mental well-being [9–11] and decreases the risk for psychopathology [4, 12], especially depression [13–19]. Perceiving ourselves as socially connected with others can prevent depression even in the presence of other known risk factors (e.g., early trauma) [13, 14, 16]. Also, people with depression who present high levels of social support show a better prognosis [17, 18] and higher quality of life during the course and treatment of the disorder [19].
However, the positive effect of social support on mental health varies significantly among different people [20, 21]. Perceiving interactions as supportive (i.e., perceived social support) have a stronger effect on mental health outcomes than objective features of social support such as network size, frequency of contact with significant others, or material support (i.e., received support) [20, 22, 23].
In this context, attachment theory provides a productive approach to understand the variability in the effect of social support; specifically, the way different attachment styles shape both the perception and the experience of social support [3, 24, 25].
Attachment Theory
Attachment theory posits that human beings are born with a psychobiological system -the attachment system- whose main role is to regulate stress and interpersonal relationships across the lifespan [1, 2].
In children, the experience of stress activates the attachment system, motivating the child´s proximity-seeking behaviours (e.g., crying) to significant others (attachment figures). From the caregiver´s point of view, this request activates her caregiving system: a set of behaviours to regulate the child’s distress [26].
The repetition of these interactions generates a system of social expectations in children: an “internal model” [27] of how relationships work. This model set the basis for a pattern of attachment strategies, also called attachment styles in adulthood [27]. According to longitudinal studies [28, 29], attachment has a fundamental role during the whole lifespan and can be measured throughout life with a 69%–75% concordance between attachment styles during childhood to adulthood.
Four attachment styles have been identified: secure, insecure-avoidant, insecure-anxious, and disorganised [29]. In short, people with secure attachment can show signs of their distress and look for help, expecting that others will be available to help and be actually helpful. Avoidant attachment styles are characterised by hidden distress, even when physiological signs of stress are present [30]. People with avoidant attachment style tend to be emotionally overregulated: visible stress signals are suppressed to keep the closeness with the attachment figure. This behaviour is believed to be rooted in fear of others’ rejection in front of negative emotion [2]. Attachment avoidance implies efforts to maintain distance from others, expressed in compulsive self-reliance and omission of help-seeking in front of stressful situations [2].
In contrast, anxious attachment is expressed in an intense need to be close to attachment figures, high anxiety levels upon separation, and a general emotional under-regulation. It is also characterised by an exaggerated expression of distress, excessive pursuit of other’s care, and a constant preoccupation that others will not be available when needed [2].
Lastly, people with disorganised attachment orientation show an inconsistent pattern of attachment activation-deactivation as a product of repeated experiences with threatening caregiving figures [29].
Hence, different attachment styles can potentially shape the experience of interpersonal relationships. Then, it becomes relevant to ask about the role different attachment styles have in the perception of social support as explained below.
Attachment, Social Support, and Depression in the COVID-19 Context
The effect of attachment styles on perceived social support has been extensively studied [31–33]. Securely attached individuals perceive their relationships as more supportive and are generally more satisfied with the received support [32, 33]. By contrast, non-securely attached individuals report low availability of supportive figures and less satisfaction in social interactions [24, 34]. Specifically, people showing anxious attachment styles tend to initially idealise supportive figures, but they become easily disappointed, remaining with feelings of hopelessness [31, 35]. In opposition, avoidant attachment has been related to feelings of discomfort when depending on others for support, suppressing the expression of distress, and support-seeking behaviours [31]. In conclusion, attachment styles influence the way individuals experience social support.
As previously mentioned, the positive effect of social support on mental health is well documented but the characteristics of the individual differences in this relationship are still unexplored. It is relevant to understand these differences to progress in the study and treatment of mental health disorders, particularly in mood disorders like depression. Depression and depressive symptoms have been established as one of the main priorities in health research [36] due to its high and increasing prevalence and long-term consequences [37].
In the present context of the COVID-19 pandemic, depression has become of the greatest public health concern as its incidence has dramatically risen [38, 39]. The deep changes in daily social dynamics imposed by the pandemic are one of the contextual aspects of this increment [39, 40]. In this context, the role of attachment in the relationship between social support and depression becomes exceptionally relevant. Particularly, since the current COVID-19 pandemic is a known factor of stress [39, 41, 42]. As such, the pandemic has the potential to activate the attachment system [43]. In Figure 1, we offer a model for understanding the plausible effect of COVID-19 pandemic on attachment, social support, and the link with mental health outcomes such as depressive symptoms.
FIGURE 1
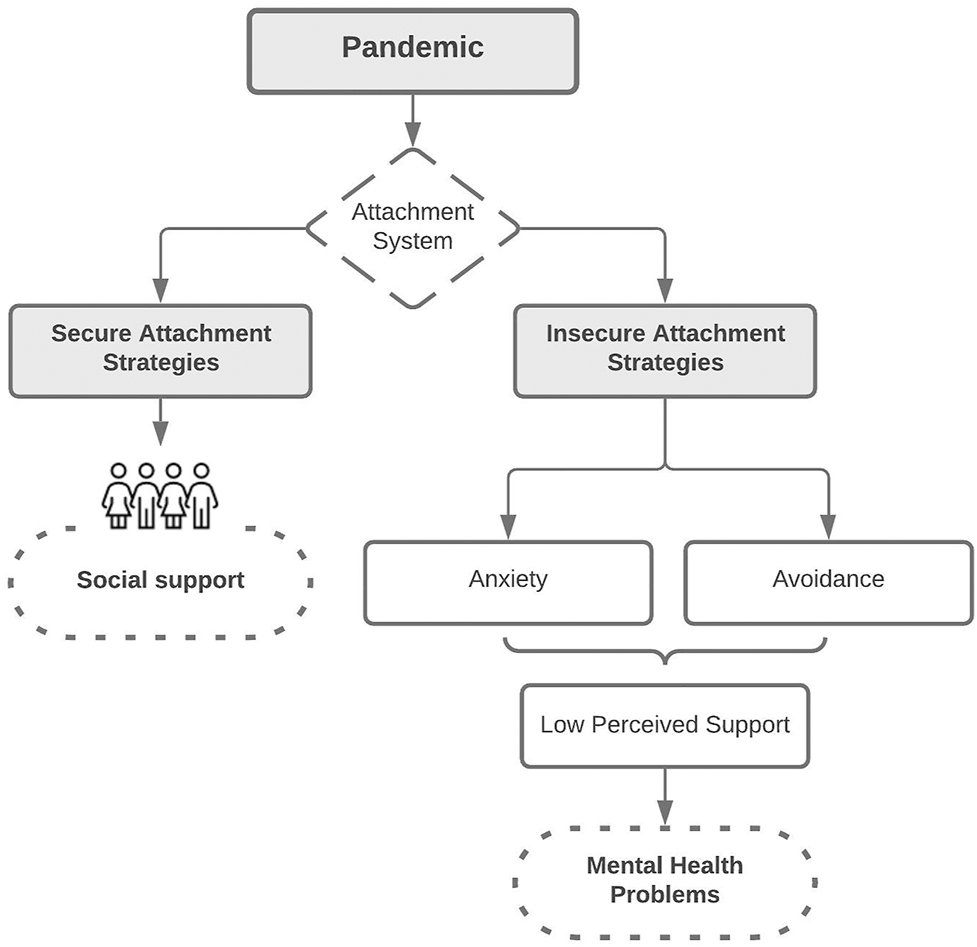
Model possible effects of the COVID-19 pandemic on attachment, social support and its relationship with mental health. Chile, 2021.
In insecurely attached individuals, the stress activation may result in either a hyperactivation of the attachment system (anxious attachment style) and excessive dependence on others or deactivation of the attachment system (avoidant attachment style) and compulsive self-reliance. In both cases, as discussed above, the experience of support from others would be negatively altered.
In a secure attachment, the activation of the attachment system and the consequent help-seeking behaviours can help look for social contact and positively use those social interactions. However, the range of measures to protect public health includes social distancing and social isolation as key prevention of COVID-19 incidence. In this context, even securely attached people who could benefit from social support in normal conditions cannot rely on their usual stress regulation strategies. Thus, the usual strategies to deal with stress are unavailable, leading the stress systems to continue to be activated.
In this scenario, secure attachment strategies are not necessarily helpful, and therefore insecure attachment strategies may get activated, which, in turn, impede the perception of social support. This process has the potential to affect mental health negatively.
The Present Study
Although there is growing evidence for the role of social support and attachment in mental health [25, 44–46], and particularly in depression [46, 47], no study to date has investigated the moderating role of attachment in the relationship between social support and depression in the context of COVID-19 pandemic. Reports show that the pandemic sanitary procedures (e.g., social distancing, repeated lockdowns, school closures) and the fear of contracting the virus among other precautionary measures have heavily impacted mental health [39, 48, 49].
Chilean circumstances have been particularly challenging. First, the pandemic started above a disrupted social context due to the 2019 social outbreak that has had important social, political and economic consequences [50], which are known risk factors for mental health [51]. Second, since mid-March 2020 Chile adopted severe restrictions on movement and social contact [52] with already known negative consequences on people’s mental health [53]. Third, because of both sanitary and social crisis, a large percentage of the population has faced serious economic difficulties [52].
Therefore, the present study aims to explore the predictive role of social support on depressive symptoms and the moderating role of attachment styles in the association between social support and depressive symptomatology.
Based on the previous literature [3, 25, 44, 47, 54], we hypothesised that securely attached individuals are more likely to display support seeking behaviours and that these strategies will positively influence their mental health. In contrast, insecurely attached individuals (either anxious or avoidant) under stress tend to isolate and behave in a compulsively self-reliant way; therefore, they will not look for help from others, impeding the benefit from social support.
Based on the evidence mentioned above, we expect to find 1) higher perceived social support to be associated with lower depressive symptoms; 2) higher attachment security to be associated with lower depressive symptoms, and 3) a moderating role of attachment in the association between social support and depressive symptomatology.
Methods
Participants and Procedure
One hundred and eighty-eight participants answered the set of online questionnaires and were included in the study analyses (N women = 148) during December 2020 and January 2021 (i.e., after 9 months of severe restrictions to social contact and during one of the strict lockdown periods). Five participants left an item blank on one of the self-reported scales. These missing values were substituted by the mean series method, using the mean of the values answered by the participant on the same scale. The sample’s mean age was 39.78 (SD = 14.72), ranging between 18 and 80 years old. 87.7% of participants reported having completed undergraduate or postgraduate education. Analysis related to sociodemographic information and the study variables is available in the Supplementary File S1.
Participants were invited to voluntarily join the study through different online platforms. All participants agreed through informed consent, which was approved on 12/29/2020 by the Ethics Committee of Universidad del Desarrollo. As retribution for participating, three gift cards valued at $100.000 CLP (around $120 US) were raffled at the end of the data collection.
The sample size was previously calculated through power analysis using the G*Power program. Anticipating an effect size of 0.15, p-value > 0.05 and B = 0.95, the minimum sample size required was N = 129. Questionnaires were displayed on the Survey monkey online platform (https://es.surveymonkey.com/). The whole survey took approximately 10–15 min for participants to complete. Only participants with completed surveys were considered as part of this study.
Instruments
Participants were asked to complete the following three scales. Further details of these instruments and data analysis plan are available in the Supplementary File S1.
The Medical Outcome Study Social Support Survey (MOSS; [55]) measures perceived social support and it is validated for the Chilean population [56]. This 18 items instrument uses a 5-point Likert scale (from 1 = Never; to 5 = Always) and an additional item assessing social network size. MOSS includes five dimensions: positive social interactions, affectionate support, instrumental support, emotional/informational support, and the social network size.
The Experiences in Close Relationship Scale Short Form [57] was adapted to measure adult attachment in general relationships (Adaptation process in Supplementary File S2). The modified version of the ECR-S used in this study has 12 items with seven response levels (from 1 = strongly disagreer; to 7 = strongly agree). The instrument allows to obtain an index of anxious and avoidant attachment for respondents.
The Beck Depression Inventory-Short Form (BDI-SF; [58]) measures depressive symptoms. We used the version validated for the Chilean population [59], and shows good reliability and validity in various populations [58, 59].
Results
Association Between Social Support and Depressive Symptoms
The linear regression analysis evidenced a significant negative association between social support and reported depressive symptoms (F(1,186) = 33.971, p < 0.001) with a = 0.154. Specifically, for each increasing point of perceived social support, reported depressive symptoms were reduced by −0.178 points (see Figure 2).
FIGURE 2
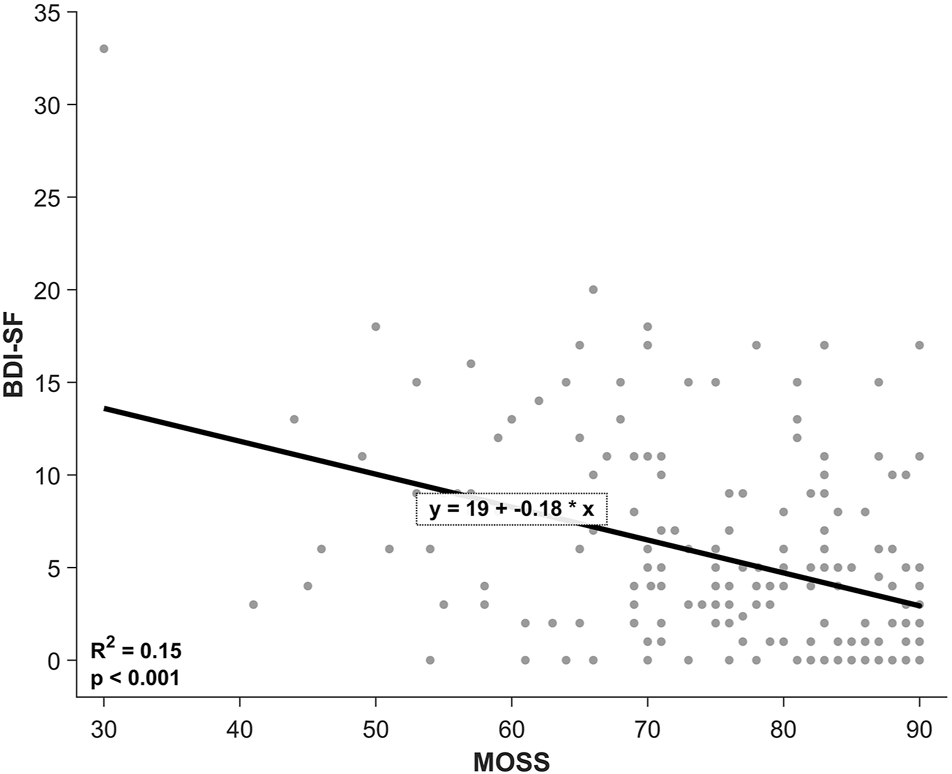
Linear regression between social support and depression. Chile, 2021.
To explore the differential effect of each social support dimension on reported depressive symptoms a multiple linear regression was run. This model (F(5,176) = 7.469, p < 0.01, = 0.175), revealed that positive social interactions (b = −0.341, t(181) = −2.177, p = 0.031) was the only significant predictor of lower depressive symptoms among the other social support dimensions (all other p-values > 0.05, See Table 1 for details).
TABLE 1
| Model | Non-standardized coefficients | Standardized coefficients | t | p-value | |
|---|---|---|---|---|---|
| B | Standard error | Beta | |||
| Constant | 18.63 | 2.57 | 7.26 | <0.001* | |
| MOSS PSIa | −0.34 | 0.16 | −0.32 | −2.18 | 0.031* |
| MOSS ASb | −0.28 | 0.26 | −0.10 | −1.04 | 0.299 |
| MOSS ISc | −0.03 | 0.13 | −0.02 | −0.23 | 0.816 |
| MOSS EISd | 0.11 | 0.23 | 0.06 | 0.45 | 0.650 |
| Person’s social network | −0.15 | 0.09 | −0.12 | −1.60 | 0.112 |
Analysis of the effect of dimensions of social support on depressive symptoms. Chile, 2021.
Positive Social Interactions.
bAffectionate Support.
cInstrumental Support.
dEmotional/Informational Support.
* Statistically significant (p < 0.05).
Association Between Attachment and Depressive Symptoms
A multiple linear regression was run to test the relationship between attachment and reported depressive symptoms. Importantly, these two dimensions of attachment insecurity evidenced no correlation (r = 0.103, p = 0.16). The regression showed a significant and positive relationship between depression and ECR-S attachment styles (F(1,185) =19.786, p < 0.01) with a = 0.176. Importantly, both attachment styles resulted as significant coefficients in this model, being avoidance (b = 0.336, t(187) = 5.041, p < 0.01) a slightly stronger predictor than anxiety (b = 0.192, t(187) = 3.218, p < 0.01). Therefore, higher levels of these attachment styles (and therefore, higher levels of attachment insecurity) are related with higher levels of reported depressive symptoms.
Moderating Effect of Attachment Styles on the Relationship Between Social Support And Depression
A moderated moderation was run to test the role of the two attachment dimensions on the relationship between perceived social support and depression (See a representation in Supplementary File S3). Under this aim, social support scores, insecure attachment dimensions and all the interactions among these predictors were included to explain depression score variance.
As shown in Table 2, this analysis evidenced a significant simple effect of avoidance (t(180) = 2.671, p = 0.01). The model also showed significant interactions between avoidance and social support (t(180) = −2.854, p < 0.01), and between the two insecure attachment dimensions (t(180) = −2.583, p = 0.01). Importantly, the third order interaction with the relevant independent variable and the two moderators was also significant (t(180) = 2.914, p < 0.01). This interaction explained a rather small but significant increase in depression variance, Δ = 0.03, F(1,180) = 8.49, p < 0.01. Thus, anxiety and avoidance attachment styles are significant moderators of the relationship between social support and depression.
TABLE 2
| Model Summary | Analysis | Analysis with covariants | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Model | R2 | MSE | F | p-value | R2 | MSE | F | p-value | ||
| 0.31 | 20.36 | 11.69 | <0.001* | 0.35 | 19.37 | 10.80 | <0.001* | |||
| Coefficient | SE | t | p-value | Coefficient | SE | t | p-value | |||
| Constant | −52.20 | 37.72 | −1.38 | 0.168 | −36.93 | 37.94 | −0.97 | 0.332 | ||
| MOSS | 0.71 | 0.46 | 1.55 | 0.124 | 0.55 | 0.47 | 1.19 | 0.236 | ||
| ECR-S avoidant | 4.24 | 1.60 | 2.67 | 0.008* | 3.63 | 1.60 | 2.26 | 0.025* | ||
| MOSS x ECR-S avoidant | −0.06 | 0.02 | −2.85 | 0.005* | −0.05 | 0.02 | −2.37 | 0.019* | ||
| ECR-S anxious | 2.77 | 1.67 | 1.66 | 0.100 | 2.48 | 1.70 | 1.46 | 0.145 | ||
| MOSS x ECR-S anxious | −0.04 | 0.02 | −1.83 | 0.070 | −0.03 | 0.02 | −1.59 | 0.114 | ||
| ECR-S avoidant x ECR-S anxious | −0.18 | 0.07 | −2.58 | 0.011* | −0.17 | 0.07 | −2.29 | 0.023* | ||
| MOSS x ECR-S avoidant x ECR-S anxious | 0.003 | 0.001 | 2.91 | 0.004* | 0.002 | 0.001 | 2.55 | 0.012* | ||
| Age | −0.07 | 0.02 | −3.18 | 0.009* | ||||||
| Educational level | −0.23 | 0.41 | −0.56 | 0.580 | ||||||
| Conditional effects | Effect | SE | t | p-value | Effect | SE | t | p-value | ||
| Levela | ECR-S avoidant | ECR-S anxious | ||||||||
| Low | Low | −0.10 | 0.08 | −1.35 | 0.180 | −0.13 | 0.08 | −1.58 | 0.117 | |
| Low | Medium | −0.10 | 0.05 | −1.89 | 0.061 | −0.13 | 0.05 | −2.36 | 0.019* | |
| Low | High | −0.10 | 0.07 | −1.32 | 0.187 | −0.13 | 0.07 | −1.81 | 0.071 | |
| Medium | Low | −0.19 | 0.05 | −3.81 | <0.001* | −0.19 | 0.05 | −3.91 | <0.001* | |
| Medium | Medium | −0.10 | 0.03 | −3.02 | 0.003* | −0.12 | 0.03 | −3.55 | <0.001* | |
| Medium | High | −0.01 | 0.05 | −0.29 | 0.775 | −0.05 | 0.05 | −0.97 | 0.333 | |
| High | Low | −0.28 | 0.05 | −5.70 | <0.001* | −0.25 | 0.05 | −5.43 | <0.001* | |
| High | Medium | −0.11 | 0.04 | −3.05 | 0.003* | −0.11 | 0.03 | −3.42 | <0.001* | |
| High | High | 0.07 | 0.06 | 1.22 | 0.223 | 0.03 | 0.05 | 0.56 | 0.575 | |
Moderated moderation model. Chile, 2021.
ECR-S avoidant and anxious scales share three levels: low, medium and high. Mean scores for each level is different for analyzes with and without control for covariates.
*Statistically significant (p < 0.05).
As reported above, educational level and age resulted in significant correlations with self-reported depression symptoms. Therefore, a new moderated moderation model was run including these two variables as covariates to control for their possible effect. This model evidenced the same significant effects; the simple effect of avoidance and the interaction between this attachment style with social support, and the two insecure attachment dimensions. Importantly, the three order interaction of social support, anxiety and avoidant attachment style was also significant. Regarding the covariates, educational level did not reach the level of significance while age did (t(178) = −3.176, p = 0.01). As expected, this model still explained a small and significant portion of depression variance, Δ = 0.02, F(1,178) = 6.48, p = 0.01.
Through the exploration of the three-way interaction of the model, it is observed that insecure attachment levels (i.e., attachment avoidance and anxiety) impacted the relationship between social support and depression in five different combinations (see Figure 3). Therefore, as detailed in Table 2, insecure attachment is a relevant moderator for low and medium levels of avoidance together with low and medium levels of anxiety. Also, for medium levels of both insecure styles, and for high levels of avoidance together with low and medium levels of anxious attachment. These conditional effects evidenced that the negative relationship between social support and depressive symptoms is effective only for certain profiles of insecure attachment. Interestingly, participants scoring high on both avoidant and anxious style have a slight increase of depressive symptoms related to higher levels of social support. Although this result did not reach a significant level, it is important to consider in further studies.
FIGURE 3
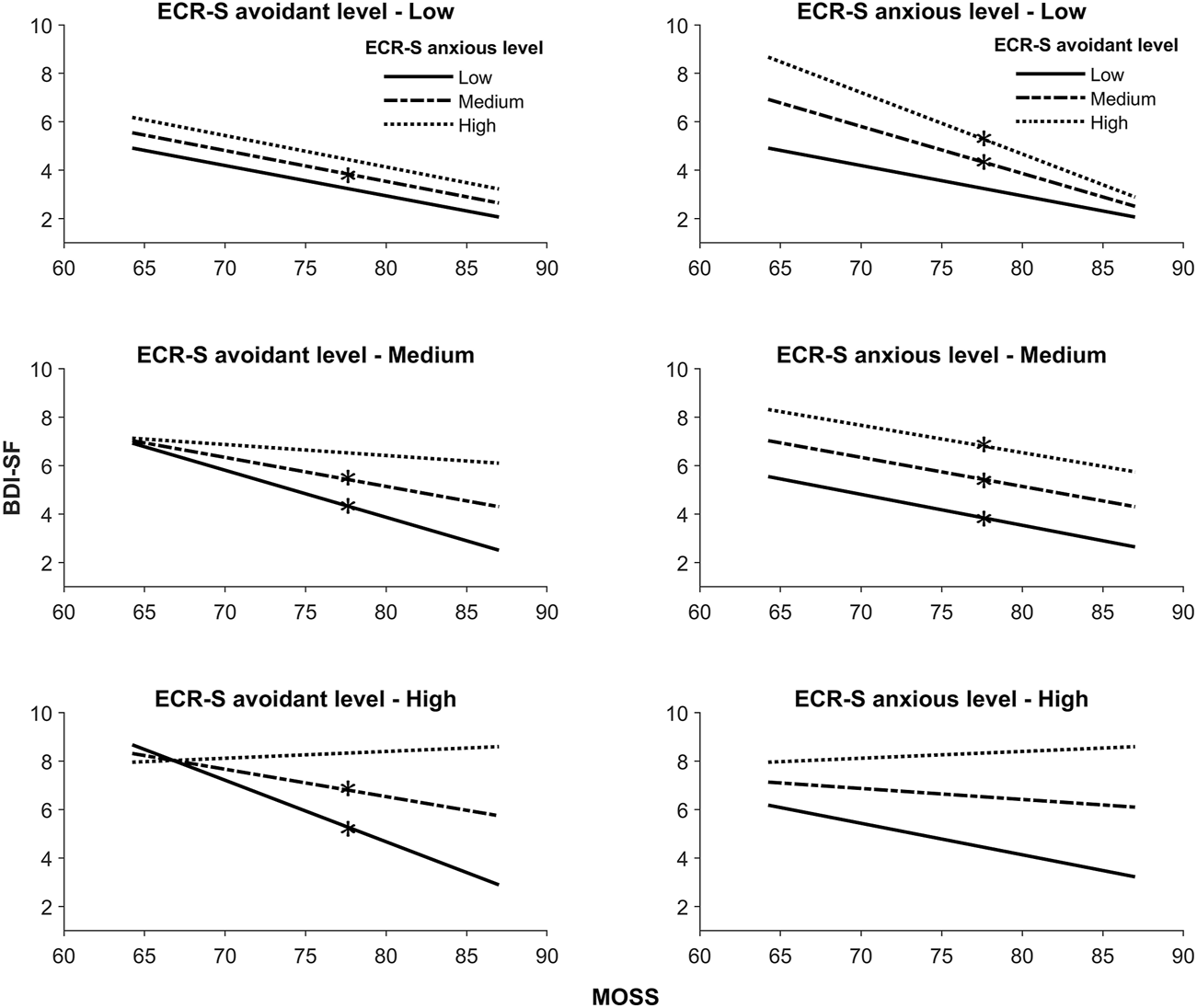
Visual result of moderate moderation. Chile, 2021.
Discussion
We examined the relationship between social support and depression during the COVID-19 pandemic and the role of attachment in this association. As expected, we found that depressive symptoms were lower in people securely attached and in those perceiving themselves as socially supported. In addition, we found that attachment modulated the effect of social support on depressive levels. These associations were not explained by sociodemographic characteristics.
Specifically, lower levels of positive social interactions and higher attachment anxiety and attachment avoidance predicted the greatest depressive symptomatology. More importantly, we found a three-way interaction suggesting a crucial role of attachment styles in the effect of social support on depression. Regarding the association between social support and depression, our findings further corroborated the increasing evidence on the role of social support as a protective factor for depression [60, 61]. More specifically, the dimension “positive social interaction” was the strongest predictor of lower depressive symptoms. A possible explanation for this result might be the evidence that the positive social interactions dimension of social support is almost equivalent to the emotional support dimension [56], which, in turn, has shown to be the most important protective factor against depression in adults [62].
Another important finding is the association between attachment and depression. Specifically, higher levels of attachment anxiety and avoidance—and therefore, levels of attachment insecurity- were related to higher levels of depressive symptomatology. These results are in line with a body of evidence showing the concomitance of depression and attachment insecurity. Several meta-analyses have shown that insecurely attached people are at greater risk for psychopathologies like depression, whilst attachment security constitutes a protective factor that prevents the development of psychopathology [63, 64]. A recent meta-analysis [63] concluded that attachment insecurity and depressive symptoms have consistently been shown to be associated (in both longitudinal and cross-sectional studies). The authors state that this association can be explained considering several factors: genetics, as in shared genetic vulnerability for attachment insecurity and depression; cognitive factors, with an internal working model of attachment as the base of dysfunctional cognitions, the core of depression according to Beck [65]; socio-emotional factors, such as social abilities and emotion regulation; and sociocultural factors, such as shared socio-ecological risk environment [63].
As noted, attachment and depression are indeed related, and therefore it is pivotal to consider this association when linking social support to depression. The latter brings us to our third hypothesis: the role of attachment in the association between social support and depression. In this regard, as expected, we found a three-way interaction between social support, attachment avoidance, and attachment anxiety in predicting depressive symptoms. Furthermore, this finding suggests that higher levels of social support affect depression that gets modulated by the levels of attachment security. That is to say; social support can have a positive impact and act as a protective factor for depression if there is a presence of security in attachment. These results are novel, and they contribute to the current literature with a more comprehensive understanding of the mechanisms underlying the effect of social support on depression.
This combination of findings supports the conceptual model presented in the introduction section, confirming that social support can be more helpful in preventing mental health problems in people with secure attachment and less useful in people with attachment insecurity.
People with an insecure attachment style perceive their social network as less supportive than people with a secure attachment style [44]. This perceived lack of support can, in turn, be associated with more depressive symptoms. By contrast, people with secure attachment benefit more from interpersonal relationships [54], and high-quality interpersonal relationships are a known protective factor for depression [61].
Regarding specific attachment styles, on the one hand, avoidant attachment is characterised by fear of intimacy and discomfort with closeness [66], being typical for avoidant people to be unhappy with close relationships. Furthermore, evidence has continually found depressive symptoms linked to a lack of social interaction [67, 68]. Indeed, social isolation has been postulated as one of the causes of depression [69–71]. On the other hand, attachment anxiety has been linked with biased and often negative perceptions of social support [24, 72]. People with anxious attachment styles are characterised by interpersonal suffering regardless of whether or not they have adequate social support [66]. These negative perceptions of social support might undermine the potential positive effects of social support on mental health.
Additionally, the effect of social support on mental health has been often explained using the stress-buffering model [73], which states that quality interpersonal relationships act as protective factors of the detrimental effects of stress, mainly through neuroendocrinological mechanisms (e.g., the presence of a significant other dampens the HPA axis stress response) that would modulate the response in front of stressors diminishing depressive symptoms and improving mood [17, 19]. Our findings align with the buffering stress model, but they go beyond that model by suggesting a fundamental role of attachment in those associations. Since attachment is mainly a system for regulating stress through interpersonal relationships [2], individual differences in attachment strategies are very likely to modulate how people experience support from their social environment.
Finally, an unexpected finding was the effect of high levels of anxiety and avoidance simultaneously, which showed to revert the association between social support and depression. When both scores were concurrently high, great levels of social support predicted high levels of depressive symptoms. This result can be explained considering the so-called “fearful-avoidant” attachment style [74], a specific pattern described in individuals who simultaneously reject engaging in close relationships and have an extreme necessity of being close and loved by others [74, 75]. Even though the specificity of this pattern is still controversial [74, 75], evidence has shown fearful avoidance to be related to severe difficulties in emotional regulation within relationships. For example, people with fearful avoidant attachment show a more negative perception of others’ support [76] and less commitment and satisfaction in romantic relationships [77, 78]. In this way, these results may be related to the negative experience of close relationships that can trigger interpersonal conflict. It is known that some people can score high in social support and at the same time present negative health outcomes [79, 80], especially when they experience their social network as containing both positive and negative experiences (e.g., experienced interpersonal conflict).
In sum, our results confirm the role of social support on depression and add to the current literature by connecting attachment security as an essential factor to include in our current understanding of relationships and mental health.
Although greater levels of social support were associated with lower levels of depression we cannot definitively conclude that social support alone accounted for this effect. Other uncontrolled variables, such as the type of householding during the pandemic lockdown, levels of physical activity, concomitant chronic or other unknown variables may have contributed to this effect. In addition, more precise measurements (i.e., not only self-report questionnaires) of our variables than what we used and further measurements over time would be needed to confirm these associations.
Our study variables are complex, and they relate to several psychosocial phenomena. Future studies should explore the role of other individual differences that might influence the perception of social support (e.g., personality) and control factors that affect depressive symptoms (e.g., diagnosis and treatment). Other limitations of our work include the sampling method (snowball convenience) and the lack of specific tools measuring aspects related to the COVID-19 pandemic (e.g., stress levels).
Taken together, our findings demonstrate that attachment has a key role in the individual differences in the effect of social support on depressive symptoms. Health interventions for depression have not yet addressed the therapeutic potential of social relationships efficiently [81] despite the amount of evidence showing its role in depression [60, 62]. Our results suggest that integrating attachment theory within social support approaches can provide a compelling framework for studying and developing treatments considering the role of interpersonal relationships in depression in a more meaningful and applicable way.
Further research might explore the clinical usefulness of these findings, analysing the evolution of the variables assessed in this study throughout therapeutic processes.
Statements
Ethics Statement
The studies involving human participants were reviewed and approved by the Comité de Ética, Universidad del Desarrollo. The patients/participants provided their written informed consent to participate in this study.
Author Contributions
Designed the research: SC-C, AV-C, and JS. Supervised research: SC-C and AR. Perform research: AV-C, SC-C, and CA-R. Analyzed the data: AV-C. Wrote the manuscript: SC-C, CA-R, AR, and AV-C.
Funding
The present work was financed by Agencia Nacional de Investigación y Desarrollo (ANID, Chile) through FONDECYT regular No. 1190610 to AR. This study also received funding from ANID—Iniciativa Científica Milenio, Instituto Milenio para la Investigación en Depresión y Personalidad (MIDAP) and FONDECYT No. 1221538. The funder was not involved in the study design, collection, analysis, interpretation of data, the writing of this article or the decision to submit it for publication.
Acknowledgments
We thank Franco Medina for useful discussions.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.ssph-journal.org/articles/10.3389/ijph.2022.1604401/full#supplementary-material
References
1
Bowlby J . Attachment and Loss. New York: Basic Books (1969).
2
Shaver PR Mikulincer M . Adult Attachment Strategies and the Regulation of Emotion. In: Handbook of Emotion Regulation [Internet]. New York, US: The Guilford Press (2007). p. 446–65.
3
Florian V Mikulincer M Bucholtz I . Effects of Adult Attachment Style on the Perception and Search for Social Support. J Psychol (1995) 129(6):665–76. 10.1080/00223980.1995.9914937
4
Thompson RA Goodvin R . Social Support and Developmental Psychopathology. In: Developmental Psychopathology [Internet]. Hoboken, NJ, USA: John Wiley & Sons (2016). p. 1–50. 10.1002/9781119125556.devpsy403
5
Harandi TF Taghinasab MM Nayeri TD . The Correlation of Social Support with Mental Health: A Meta-Analysis. Electron Physician (2017) 9(9):5212–22. 10.19082/5212
6
Uchino BN Bowen K Kent R . Social Support and Mental Health. In: Encyclopedia of Mental Health. Cambridge, Massachusetts, US: Academic Press (2016). p. 189–95. 10.1016/b978-0-12-397045-9.00117-8
7
Ozbay F Fitterling H Charney D Southwick S . Social Support and Resilience to Stress across the Life Span: a Neurobiologic Framework. Curr Psychiatry Rep (2008) 10(4):304–10. 10.1007/s11920-008-0049-7
8
Costa-Cordella S Arevalo-Romero C Parada FJ Rossi A . Social Support and Cognition: A Systematic Review. Front Psychol (2021) 12:637060. 10.3389/fpsyg.2021.637060
9
Cohen S Underwood LG Gottlieb BH . Social Support Measurement and Intervention: A Guide for Health and Social Scientists [Internet]. Oxford, UK: Oxford University Press (2000). p. 368.
10
Uchino BN . Social Support and Physical Health: Understanding the Health Consequences of Relationships. New Haven, Connecticut, US: Yale University Press (2004).
11
Gottlieb BH Bergen AE . Social Support Concepts and Measures. J Psychosomatic Res (2010) 69(5):511–20. 10.1016/j.jpsychores.2009.10.001
12
Sperry DM Widom CS . Child Abuse and Neglect, Social Support, and Psychopathology in Adulthood: a Prospective Investigation. Child Abuse Neglect (2013) 37(6):415–25. 10.1016/j.chiabu.2013.02.006
13
Stice E Ragan J Randall P . Prospective Relations between Social Support and Depression: Differential Direction of Effects for Parent and Peer Support?J Abnormal Psychol (2004) 113(1):155–9. 10.1037/0021-843X.113.1.155
14
Wight RG Botticello AL Aneshensel CS . Socioeconomic Context, Social Support, and Adolescent Mental Health: A Multilevel Investigation. J Youth Adolescence (2006) 35(1):109–20. 10.1007/s10964-005-9009-2
15
Ellonen N Kääriäinen J Autio V . Adolescent Depression and School Social Support: a Multilevel Analysis of a Finnish Sample. J Community Psychol (2008) 36(4):552–67. 10.1002/jcop.20254
16
Dingfelder HE Jaffee SR Mandell DS . The Impact of Social Support on Depressive Symptoms Among Adolescents in the Child Welfare System: A Propensity Score Analysis. Child Youth Serv Rev (2010) 32(10):1255–61. 10.1016/j.childyouth.2010.04.016
17
Wang X Cai L Qian J Peng J . Social Support Moderates Stress Effects on Depression. Int J Ment Health Syst (2014) 8(1):41. 10.1186/1752-4458-8-41
18
Ren P Qin X Zhang Y Zhang R . Is Social Support a Cause or Consequence of Depression? A Longitudinal Study of Adolescents. Front Psychol (2018) 9:1634. 10.3389/fpsyg.2018.01634
19
Cruwys T Alexander Haslam S Dingle GA Jetten J Hornsey MJ Desdemona Chong EM et al Feeling Connected Again: Interventions that Increase Social Identification Reduce Depression Symptoms in Community and Clinical Settings. J Affective Disord (2014) 159:139–46. 10.1016/j.jad.2014.02.019
20
Kaul M Lakey B . Where Is the Support in Perceived Support? the Role of Generic Relationship Satisfaction and Enacted Support in Perceived Support's Relation to Low Distress. J Soc Clin Psychol (2003) 22(1):59–78. 10.1521/jscp.22.1.59.22761
21
DiMatteo MR . Social Support and Patient Adherence to Medical Treatment: a Meta-Analysis. Health Psychol (2004) 23(2):207–18. 10.1037/0278-6133.23.2.207
22
Dunkel-Schetter C Bennett TL . The Availability of Social Support and its Activation in Times of Stress. Social support: interactional view (1990) 1990:1.
23
Lakey B Heller K . Social Support from a Friend, Perceived Support, and Social Problem Solving. Am J Community Psychol [Internet] (1988) 16(6):811–24. 10.1007/BF00930894
24
Collins NL Feeney BC . Working Models of Attachment Shape Perceptions of Social Support: Evidence from Experimental and Observational Studies. J Personal Soc Psychol (2004) 87(3):363–83. 10.1037/0022-3514.87.3.363
25
Mikulincer M Shaver PR . An Attachment and Behavioral Systems Perspective on Social Support. J Soc Personal Relationships (2009) 26(1):7–19. 10.1177/0265407509105518
26
George C Solomon J . The Caregiving System: A Behavioral Systems Approach to Parenting. In: Handbook of Attachment: Theory, Research, and Clinical Applications. 2nd ed. New York, US: Guilford Press (2008). p. 833–56.
27
Bretherton I Munholland KA . Internal Working Models in Attachment Relationships: Elaborating a central Construct in Attachment Theory. In: Handbook of Attachment: Theory, Research, and Clinical Applications. 2nd ed. New York, US: Guilford Press (1999). p. 102–27.
28
Fonagy P Steele M Moran G Steele H Higgitt A . Measuring the Ghost in the Nursery: An Empirical Study of the Relation between Parents' Mental Representations of Childhood Experiences and Their Infants' Security of Attachment. J Am Psychoanal Assoc (1993) 41(4):957–89. 10.1177/000306519304100403
29
Ainsworth MDS Blehar MC Waters E Wall SN . Patterns of Attachment: A Psychological Study of the Strange Situation. Mahwah, New Jersey, US: Lawrence Erlbaum Associates (2015).
30
Vrticka P Andersson F Grandjean D Sander D Vuilleumier P . Individual Attachment Style Modulates Human Amygdala and Striatum Activation during Social Appraisal. PLoS One (2008) 3(8):e2868. 10.1371/journal.pone.0002868
31
Collins NL Feeney BC . A Safe haven: an Attachment Theory Perspective on Support Seeking and Caregiving in Intimate Relationships. J Personal Soc Psychol (2000) 78(6):1053–73. 10.1037/0022-3514.78.6.1053
32
Sirois FM Millings A Hirsch JK . Insecure Attachment Orientation and Well-Being in Emerging Adults: The Roles of Perceived Social Support and Fatigue. Personal Individual Differences (2016) 101:318–21. 10.1016/j.paid.2016.06.026
33
Zhang X Chen X Ran G Ma Y . Adult Children’s Support and Self-Esteem as Mediators in the Relationship between Attachment and Subjective Well-Being in Older Adults. Pers Individ Dif [Internet] (2016) 97:229–33. 10.1016/j.paid.2016.03.062
34
Danielsen AG Samdal O Hetland J Wold B . School-Related Social Support and Students' Perceived Life Satisfaction. J Educ Res (2009) 102(4):303–20. 10.3200/JOER.102.4.303-320
35
Mikulincer M Birnbaum G Woddis D Nachmias O . Stress and Accessibility of Proximity-Related Thoughts: Exploring the Normative and Intraindividual Components of Attachment Theory. J Pers Soc Psychol [Internet] (2000) 78:509–23. 10.1037/0022-3514.78.3.509
36
World Health Organization. Depression and Other Common Mental Disorders: Global Health Estimates [Internet]. Geneva, Switzerland: World Health Organization (2017).
37
GBD. Global, Regional, and National Incidence, Prevalence, and Years Lived with Disability for 354 Diseases and Injuries for 195 Countries and Territories, 1990-2017: a Systematic Analysis for the Global Burden of Disease Study 2017. Lancet (2018) 392(10159):1789–858. 10.1016/S0140-6736(18)32279-7
38
Hotopf M Bullmore E O'Connor RC Holmes EA . The Scope of Mental Health Research during the COVID-19 Pandemic and its Aftermath. Br J Psychiatry (2020) 217:540–2. 10.1192/bjp.2020.125
39
Xiong J Lipsitz O Nasri F Lui LMW Gill H Phan L et al Impact of COVID-19 Pandemic on Mental Health in the General Population: A Systematic Review. J Affective Disord (2020) 277:55–64. 10.1016/j.jad.2020.08.001
40
Polack RG Sened H Aubé S Zhang A Joormann J Kober H . Connections during Crisis: Adolescents’ Social Dynamics and Mental Health during COVID-19. PsyArXiv (2021).
41
Kujawa A Green H Compas BE Dickey L Pegg S . Exposure to COVID‐19 Pandemic Stress: Associations with Depression and Anxiety in Emerging Adults in the United States. Depress Anxiety (2020) 37(12):1280–8. 10.1002/da.23109
42
Horesh D Brown AD . Traumatic Stress in the Age of COVID-19: A Call to Close Critical Gaps and Adapt to New Realities. Psychol Trauma Theor Res Pract Pol (2020) 12(4):331–5. 10.1037/tra0000592
43
Steele H . COVID-19, Fear and the Future: An Attachment Perspective. Clin Neuropsychiatry (2020) 17(2):97–9. 10.36131/CN20200213
44
Priel B Shamai D . Attachment Style and Perceived Social Support: Effects on Affect Regulation. Personal Individual Differences (1995) 19(2):235–41. 10.1016/0191-8869(95)91936-t
45
McLewin LA Muller RT . Attachment and Social Support in the Prediction of Psychopathology Among Young Adults with and without a History of Physical Maltreatment. Child Abuse Neglect (2006) 30(2):171–91. 10.1016/j.chiabu.2005.10.004
46
Kafetsios K Sideridis GD . Attachment, Social Support and Well-Being in Young and Older Adults. J Health Psychol (2006) 11(6):863–75. 10.1177/1359105306069084
47
Zhu W Wang CD Chong CC . Adult Attachment, Perceived Social Support, Cultural Orientation, and Depressive Symptoms: A Moderated Mediation Model. J Couns Psychol (2016) 63(6):645–55. 10.1037/cou0000161
48
Chidiebere Okechukwu E Tibaldi L La Torre G . The Impact of COVID-19 Pandemic on Mental Health of Nurses. Clin Ter (2020) 171(5):e399–400. 10.7417/CT.2020.2247
49
Zhou J Zogan H Yang S Jameel S Xu G Chen F . Detecting Community Depression Dynamics Due to COVID-19 Pandemic in Australia. IEEE Trans Comput Soc Syst (2021) 8:982–91. 10.1109/tcss.2020.3047604
50
Bossert TJ Villalobos Dintrans P . Health Reform in the Midst of a Social and Political Crisis in Chile, 2019-2020. Health Syst Reform (2020) 6(1):e1789031. 10.1080/23288604.2020.1789031
51
Fischman P Irarrazaval M . Debate: Mental Health, Social Crisis and the COVID‐19 Pandemic in Chile. Child Adolesc Ment Health (2020) 25(4):256–7. 10.1111/camh.12424
52
Benítez MA Velasco C Sequeira AR Henríquez J Menezes FM Paolucci F . Responses to COVID-19 in Five Latin American Countries. Health Pol Technology (2020) 9(4):525–59. 10.1016/j.hlpt.2020.08.014
53
Duarte F Jiménez-Molina Á . Psychological Distress during the COVID-19 Epidemic in Chile: The Role of Economic Uncertainty. PLoS One (2021) 16:e0251683. 10.1371/journal.pone.0251683
54
Baker JK . The Impact of Attachment Style on Coping Strategies, Identity Development and the Perception of Social Support. Christchurch, New Zealand: University of Canterbury (2006).
55
Sherbourne CD Stewart AL . The MOS Social Support Survey. Soc Sci Med (1991) 32(6):705–14. 10.1016/0277-9536(91)90150-B
56
Poblete F Glasinovic A Sapag J Barticevic N Arenas A Padilla O . Apoyo social y salud cardiovascular: adaptación de una escala de apoyo social en pacientes hipertensos y diabéticos en la atención primaria chilena. Atención Primaria (2015) 47(8):523–31. 10.1016/j.aprim.2014.10.010
57
Wilkinson RB . Measuring Attachment Dimensions in Adolescents: Development and Validation of the Experiences in Close Relationships - Revised - General Short Form. J Relat Res (2011) 2(1):53–62. 10.1375/jrr.2.1.53
58
Beck AT Rial WY Rickels K . Short Form of Depression Inventory: Cross-Validation. Psychol Rep (1974) 34(3):1184–6. 10.1177/003329417403403s01
59
Melipillán Araneda R Cova Solar F Rincón González P Valdivia Peralta M . Propiedades psicométricas del Inventario de Depresión de Beck-II en adolescentes chilenos. Terapia [Internet] (2008) 26(1):59–69. 10.4067/s0718-48082008000100005
60
Wang J Mann F Lloyd-Evans B Ma R Johnson S . Associations between Loneliness and Perceived Social Support and Outcomes of Mental Health Problems: a Systematic Review. BMC Psychiatry (2018) 18(1):156. 10.1186/s12888-018-1736-5
61
Santini ZI Koyanagi A Tyrovolas S Mason C Haro JM . The Association between Social Relationships and Depression: a Systematic Review. J Affective Disord (2015) 175:53–65. 10.1016/j.jad.2014.12.049
62
Gariépy G Honkaniemi H Quesnel-Vallée A . Social Support and protection from Depression: Systematic Review of Current Findings in Western Countries. Br J Psychiatry (2016) 209(4):284–93. 10.1192/bjp.bp.115.169094
63
Spruit A Goos L Weenink N Rodenburg R Niemeyer H Stams GJ et al The Relation between Attachment and Depression in Children and Adolescents: A Multilevel Meta-Analysis. Clin Child Fam Psychol Rev (2020) 23(1):54–69. 10.1007/s10567-019-00299-9
64
Colonnesi C Draijer EM Jan J. M. StamsM Stams GG Van der Bruggen CO Bögels SM Noom MJ . The Relation between Insecure Attachment and Child Anxiety: a Meta-Analytic Review. J Clin Child Adolesc Psychol (2011) 40(4):630–45. 10.1080/15374416.2011.581623
65
Beck AT . Cognitive Models of Depression. Clin Adv Cogn psychotherapy: Theor Appl [Internet] (2002) 14(1):29–61.
66
Pietromonaco PR Feldman Barrett L . Attachment Theory as an Organizing Framework: A View from Different Levels of Analysis. Rev Gen Psychol (2000) 4(2):107–10. 10.1037/1089-2680.4.2.107
67
Joiner TE . In: GotlibIHHammenCL, editors. Handbook of Depression [Internet]. New York, NY, US: The Guilford Press (2002). p. 295–313.Depression in its Interpersonal Context.
68
Glass TA De Leon CFM Bassuk SS Berkman LF . Social Engagement and Depressive Symptoms in Late Life. J Aging Health (2006) 18(4):604–28. 10.1177/0898264306291017
69
Paykel ES . Life Events, Social Support and Depression. Acta Psychiatr Scand (1994) 89:50–8. 10.1111/j.1600-0447.1994.tb05803.x
70
Tennant C . Life Events, Stress and Depression: A Review of Recent Findings. Aust N Z J Psychiatry (2002) 36(2):173–82. 10.1046/j.1440-1614.2002.01007.x
71
Beck JS . Cognitive Behavior Therapy: Basics and beyond. New York, US: Guilford Press: The Guilford Press (2011).
72
Bradford SA Feeney JA Campbell L . Links between Attachment Orientations and Dispositional and Diary-Based Measures of Disclosure in Dating Couples: A Study of Actor and Partner Effects. Personal Relationships (2002) 9(4):491–506. 10.1111/1475-6811.00031
73
Rueger SY Malecki CK Pyun Y Aycock C Coyle S . A Meta-Analytic Review of the Association between Perceived Social Support and Depression in Childhood and Adolescence. Psychol Bull (2016) 142(10):1017–67. 10.1037/bul0000058
74
Shaver PR Mikulincer M . Attachment-related Psychodynamics. Attachment Hum Development (2002) 4(2):133–61. 10.1080/14616730210154171
75
Simpson JA Rholes WS . Fearful-avoidance, Disorganization, and Multiple Working Models: Some Directions for Future Theory and Research. Attachment Hum Development (2002) 4(2):223–9. 10.1080/14616730210154207
76
Forsythe LP Romano JM Jensen MP Thorn BE . Attachment Style Is Associated with Perceived Spouse Responses and Pain-Related Outcomes. Rehabil Psychol (2012) 57(4):290–300. 10.1037/a0030083
77
Banse R . Adult Attachment and Marital Satisfaction: Evidence for Dyadic Configuration Effects. J Soc Personal Relationships (2004) 21(2):273–82. 10.1177/0265407504041388
78
Pistole MC Vocaturo LC . Attachment and Commitment in College Students’ Romantic Relationships. J Coll Stud Dev [Internet] (1999) 40(6):710–20.
79
Reblin M Uchino BN Smith TW . Provider and Recipient Factors that May Moderate the Effectiveness of Received Support: Examining the Effects of Relationship Quality and Expectations for Support on Behavioral and Cardiovascular Reactions. J Behav Med (2010) 33(6):423–31. 10.1007/s10865-010-9270-z
80
Uchino BN Bowen K Carlisle M Birmingham W . Psychological Pathways Linking Social Support to Health Outcomes: a Visit with the “Ghosts” of Research Past, Present, and Future. Soc Sci Med (2012) 74(7):949–57. 10.1016/j.socscimed.2011.11.023
81
Roehrle B Strouse J . Influence of Social Support on success of Therapeutic Interventions: A Meta-Analytic Review. Psychotherapy: Theor Res Pract Train (2008) 45(4):464–76. 10.1037/a0014333
Summary
Keywords
mental health, COVID-19, depression, social support, attachment, attachment theory
Citation
Costa-Cordella S, Vivanco-Carlevari A, Rossi A, Arévalo-Romero C and Silva JR (2022) Social Support and Depressive Symptoms in the Context of COVID-19 Lockdown: The Moderating Role of Attachment Styles. Int J Public Health 67:1604401. doi: 10.3389/ijph.2022.1604401
Received
11 August 2021
Accepted
20 May 2022
Published
15 June 2022
Volume
67 - 2022
Edited by
Jutta Linder, University of Applied Sciences Emden Leer, Germany
Reviewed by
Αreti Spyropoulou, National and Kapodistrian University of Athens, Greece
Ruth Sharabany, University of Haifa, Israel
Updates
Copyright
© 2022 Costa-Cordella, Vivanco-Carlevari, Rossi, Arévalo-Romero and Silva.
This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Stefanella Costa-Cordella, stefanella.costa@mail.udp.cl; Anastassia Vivanco-Carlevari, avivanco@udd.cl
This Original Article is part of the IJPH Special Issue “The Impact of the COVID-19 Pandemic on Mental Health.”
Disclaimer
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.