 Roberto Mediavilla1,2,3*
Roberto Mediavilla1,2,3* Eduardo Fernández-Jiménez3,4
Eduardo Fernández-Jiménez3,4 Irene Martinez-Morata5,6Fabiola Jaramillo7,8Jorge Andreo-Jover1,3Inés Morán-Sánchez6
Irene Martinez-Morata5,6Fabiola Jaramillo7,8Jorge Andreo-Jover1,3Inés Morán-Sánchez6 Franco Mascayano5,9Berta Moreno-Küstner10,11Sergio Minué7José Luis Ayuso-Mateos1,2,12Richard A. Bryant13María-Fe Bravo-Ortiz1,2,3,4Gonzalo Martínez-Alés3,5
Franco Mascayano5,9Berta Moreno-Küstner10,11Sergio Minué7José Luis Ayuso-Mateos1,2,12Richard A. Bryant13María-Fe Bravo-Ortiz1,2,3,4Gonzalo Martínez-Alés3,5- 1Department of Psychiatry, Universidad Autónoma de Madrid (UAM), Madrid, Spain
- 2Centro de Investigación Biomédica en Red de Salud Mental (CIBERSAM), Madrid, Spain
- 3University Hospital La Paz Research Institute (IdiPAZ), Madrid, Spain
- 4University Hospital La Paz, La Paz, Spain
- 5Mailman School of Public Health, Columbia University, New York City, NY, United States
- 6Murcia BioHealth Research Institute, University of Murcia, Murcia, Spain
- 7Andalusian School of Public Health, Granada, Spain
- 8University of Chile, Santiago, Chile
- 9New York State Psychiatric Institute (NYSPI), New York City, NY, United States
- 10Department of Personality, Assessment, and Psychological Treatment, University of Malaga, Málaga, Spain
- 11Instituto de Investigaciones Biomédicas de Málaga, Universidad de Málaga, Málaga, Spain
- 12Fundación Biomédica, Hospital de La Princesa, Madrid, Spain
- 13School of Psychology, University of New South Wales, Kensington, NSW, Australia
Objective: To characterize the evolution of healthcare workers’ mental health status over the 1-year period following the initial COVID-19 pandemic outbreak and to examine baseline characteristics associated with resolution or persistence of mental health problems over time.
Methods: We conducted an 8-month follow-up cohort study. Eligible participants were healthcare workers working in Spain. Baseline data were collected during the initial pandemic outbreak. Survey-based self-reported measures included COVID-19-related exposures, sociodemographic characteristics, and three mental health outcomes (psychological distress, depression symptoms, and posttraumatic stress disorder symptoms). We examined three longitudinal trajectories in mental health outcomes between baseline and follow-up assessments (namely asymptomatic/stable, recovering, and persistently symptomatic/worsening).
Results: We recruited 1,807 participants. Between baseline and follow-up assessments, the proportion of respondents screening positive for psychological distress and probable depression decreased, respectively, from 74% to 56% and from 28% to 21%. Two-thirds remained asymptomatic/stable in terms of depression symptoms and 56% remained symptomatic or worsened over time in terms of psychological distress.
Conclusion: Poor mental health outcomes among healthcare workers persisted over time. Occupational programs and mental health strategies should be put in place.
Introduction
The COVID-19 pandemic outbreak has had substantial mental health impact on healthcare workers (HCWs), largely due to increases in healthcare capacity requirements driving job redeployments and extended working hours in combination with very high risk of contagion and death. Estimates from cross-sectional studies conducted during the initial pandemic outbreak suggest that between 25% and 50% of HCWs may have experienced clinically significant symptoms of anxiety or depression [1–7] and posttraumatic stress [1, 3, 7].
The extent to which the deleterious mental health effects brought about by the initial pandemic outbreak may have subsequently led to negative mid- and long-term mental health outcomes among HCWs, however, remains largely unexplored—despite important public health and clinical implications [8]. For instance, whether mental health support interventions for HCWs should be maintained in the long-term following the initial pandemic outbreak remains unexplored. Initially, it seemed plausible that a large proportion of the burden of mental health symptoms initially reported by HCWs would eventually resolve, either following cessation of exposure to the acute stressor or after adequate targeted interventions (e.g., self-care and low-intensity psychotherapeutic interventions). Nevertheless, because the initial pandemic outbreak has been followed by a series of ongoing subsequent pandemic waves that continue to strain health systems across the globe, there is a generalized concern that a substantial proportion of HCWs may be experiencing persistent mental health problems. According to the World Health Organization, reducing the long-term mental health impact of the pandemic on HCWs is considered a major clinical and public health priority. Estimating the mid- and long-term mental health impact of the COVID-19 pandemic among HCWs is paramount for occupational and mental healthcare planning purposes. In addition, identifying risk and protective factors for persistence of clinically significant mental health burden can help improve implementation of evidence-based detection and treatment strategies. For example, risk and protective factors can guide early identification and targetting of at-risk individuals for more efficient treatment resource allocation. Notwithstanding, evidence examining prevalence and predictors of persistence of mental health symptoms among HCWs from longitudinal cohort studies is scarce [9–12].
Here we used a large sample of HCWs during the 1-year period following the initial pandemic outbreak in one of the largest COVID-19 hotspots globally to [1] characterize the evolution of HCWs’ mental health status over the year following the initial pandemic outbreak, and [2] examine baseline sociodemographic and clinical characteristics associated with resolution or persistence of mental health problems over time.
Methods
Study Design, Setting, and Participants
We conducted a prospective cohort study in Spain as part of an ongoing longitudinal multi-national study [13] (https://mentalnet.cl/en/home/). We collected data through an online survey at two timepoints. Baseline assessments were performed from 24th April to 22nd June 2020 (during the initial pandemic outbreak in Spain). Follow-up assessments took place between 26th January and 8th March 2021, which in Spain coincided with the third pandemic wave and with administration of COVID-19 vaccines for the majority of HCWs.
The study participants were HCWs aged 18 years and older, recruited from different outpatient and inpatient healthcare facilities, with clinical and non-clinical duties, and not necessarily involved in the direct care of COVID-19 patients. Participation was voluntary. The snowball sampling strategy was as follows. During both the baseline and follow-up assessments, key stakeholders (e.g., hospital managers, heads of worker unions) from healthcare facilities located in the study regions (Andalusia, Madrid, and Murcia) forwarded the survey link to all HCWs. Participants were also asked to forward the survey to peers in order to enhance response rates. In addition, during the follow-up period, we sent email or telephone survey reminders to baseline participants. Participants’ personal and clinical data remained stored in separate datasets (e.g., pseudonymized), following European General Data Protection Regulation Standards. Baseline assessments are described elsewhere [14]. In this manuscript, we focus on participants who were assessed at follow-up only and on participants assessed at follow-up who had been assessed also during baseline procedures. We hereafter refer to these two subgroups as partial and full respondents, respectively.
All procedures contributing to this work comply with the Helsinki Declaration of 1975, as revised in 2013. It received approval from the Hospital La Paz Ethics Committee in Madrid (Madrid, Spain), study ID 4099, and was ratified by the local ethics committees from the participating sites.
Variables
Baseline assessments included the following COVID-19-related exposures: direct involvement in the care of COVID-19 patients (yes, no), adequate access to personal protective equipment, fear of getting infected, and fear of infecting loved ones (all rated from 0 to 3).
Both baseline and follow-up assessments included the following sociodemographic and mental health outcome variables.
Sociodemographic variables: Age in years, gender (male, female), educational level (primary, secondary, or university studies), and type of job. We collapsed job types into the following categories: physicians, nurses, health technicians (e.g., nurse, X-ray, and laboratory technicians), ancillary workers (e.g., security staff, drivers, administrative staff, and cleaning staff), other HCWs (e.g., clinical psychologists, physiotherapists, and biologists), and residential support workers (e.g., from mental health assisted living facilities, nursing homes).
Mental health outcomes: Psychological stress, as measured by the validated Spanish version of the 12-item General Health Questionnaire (GHQ-12) [15]; and probable depression symptoms, as measured by the validated Spanish version of the 9-item Patient Health Questionnaire (PHQ-9) [16]. We used widely accepted thresholds for detecting people screening positive for psychological distress (GHQ-12 higher than 2 points) [17, 18] and for depression (PHQ-9 score higher than 9 points) [19]. In addition, follow-up assessments also included posttraumatic stress disorder (PTSD) symptoms, as measured by the Spanish 5-item version of the Primary Care PTSD Screen for DSM-5 (PC-PTSD-5), where a total score higher than 2 points suggests probable PTSD [20]. The scale has been translated, but not validated in Spain.
Cronbach’s alphas were 0.87 (95 percent CI: 0.86, 0.88) for the GHQ-12 total score; 0.89 (95 percent CI: 0.88, 0.89) for the PHQ-9 total score; and 0.70 (95 percent CI: 0.68, 0.72) for the PC-PTSD-5. To control for region-level cumulative COVID-19 incidence, we calculated region-specific 14-day cumulative incidence rates 2, 4, 6, and 8 weeks after the start of the follow-up period and, as rates were stable over time, classified regions as “high” or “low” incidence depending on whether average cumulative incidence over time points fell under or over 750 cases per 100,000 based on visual examination of region-specific cumulative incidence rates (Supplementary Figures S1, S2).
Statistical Analyses
First, we removed baseline respondents who provided informed consent but did not go on to initiate the survey (n = 95). We reported categorical variables as frequencies and valid percentages, and continuous and interval variables as either mean (standard deviation [SD]), or median (interquartile range [IQR]). Descriptive statistics were calculated separately for full and partial respondents.
Then, we used multivariable mixed-effects linear and binary logistic regression models to explore the associations between baseline variables, including sociodemographic characteristics (i.e., age, gender, and educational level) and COVID-19-related exposures (i.e., direct involvement in the care of COVID-19 patients, adequate access to personal protective equipment, fear of getting infected, and fear of infecting loved ones), and follow-up mental health outcomes (i.e., psychological distress, depression symptoms, and PTSD symptoms), defined both as continuous questionnaire scores and dichotomous variables. We conducted sensitivity analyses adjusted by baseline assessments of the follow-up outcome under consideration. We used baseline GHQ-12 score for the model where follow-up PTSD was the outcome, as we did not have estimates for the latter in the baseline assessment. The GHQ-12 score, an instrument that has good convergent validity with the PC-PTSD-5 and accurately detects PTSD in primary care settings [21]. To ease the interpretability of effect estimates from binary logistic regression models (odds ratios), we dichotomized the following baseline exposure variables: adequate access to personal protective equipment (adequate vs. inadequate), fear of getting infected (not or slightly afraid vs. considerably or extremely afraid), and fear of infecting loved ones (not or slightly afraid vs. considerably or extremely afraid).
Next, we used baseline and follow-up mental health outcomes to categorize respondents into three mental health trajectories, separately for psychological distress and for depression, according to whether they screened negative at baseline and follow-up (asymptomatic stable), positive at baseline and negative at follow-up (recovering), or positive or negative at baseline and positive at follow-up (persistently symptomatic/worsening). For instance, if a respondent screened negative in the GHQ-12 and positive in the PHQ-9 at baseline, and subsequently screened positive in the GHQ-12 and negative in the PHQ-9 at follow-up, they would belong to the persistently symptomatic/worsening trajectory for psychological distress and to the recovering trajectory for depression. We selected these trajectory categories because of their potential implications for clinical practice.
Finally, we explored the association between baseline exposures and longitudinal psychological distress and depression trajectory membership, using multinomial regression models where asymptomatic stable was considered the reference category. Baseline exposures were age group, gender, educational level, direct involvement in the care of COVID-19 patients, adequate access to personal protective equipment (adequate vs. inadequate), fear of getting infected (not or slightly afraid vs. considerably or extremely afraid), and fear of infecting loved ones (not or slightly afraid vs. considerably or extremely afraid).
All models were adjusted for confounding based on prior causal knowledge, using direct acyclic graphs and backdoor criteria [22]. Region-level cumulative incidence of COVID-19 was entered in all models as a fixed factor. Likert-type variables were included as continuous for main analyses—following an accepted analytical approach [23]. (In a set of sensitivity analyses, we included them as dummy variables to assess whether main results were robust to potential model misspecification.) We did not impute missing data. All analyses were performed using packages dplyr, gtsummary, flextable, ggplot2, psych, multinom of R Studio for Mac (Version 1.2.5042).
Results
Follow-Up Mental Health Outcomes
Of 1,807 respondents who answered the survey at follow-up (between 26th January and 25th March 2021), 1,471 (81.4%) completed the entire survey, with a median response time of 21 min. Most missing data pertained to the last section of the questionnaire, suggesting that data missingness was driven by survey extension and hence largely random. Respondents who did and did not complete the survey were comparable in terms of mean age (42 vs. 40 years, respectively) and gender distribution (78% vs. 74% female, respectively). Response rates were estimated across facilities and job types and ranged from 2.7% to 100% (see Supplementary Tables S1, S2).
There were 1,058 (59%) partial respondents (i.e., assessed only at follow-up) and 749 (41%) full respondents (i.e., assessed at both baseline and follow-up). Of note, this indicates that we retained 32% of the 2,370 original baseline respondents for follow-up assessments (see Figure 1). Sociodemographic characteristics of follow-up respondents, overall and divided into full and partial respondents, are shown in Table 1. In short, full respondents were more frequently female and more likely to have completed university studies than partial respondents. Also, while most full respondents were physicians or nurses, partial respondents included a larger proportion of residential support workers.
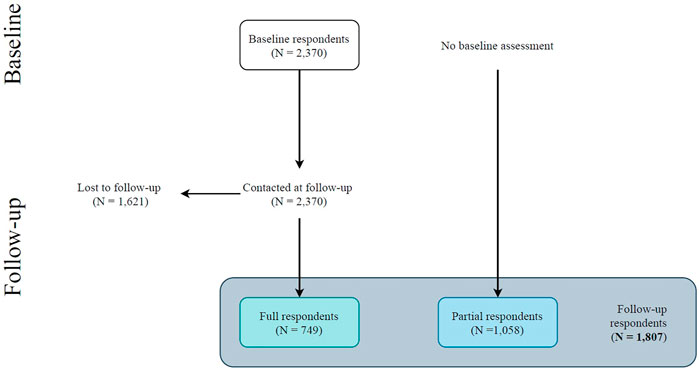
FIGURE 1. Flowchart of the participants. Follow-up respondents (N = 1,807) include participants who completed both baseline and follow-up assessments (i.e., full respondents) and participants who completed the follow-up assessment only (i.e., partial respondents) [The COVID-19 HEalth caRe wOrkErS (HEROES) Study, Spain, 2021].
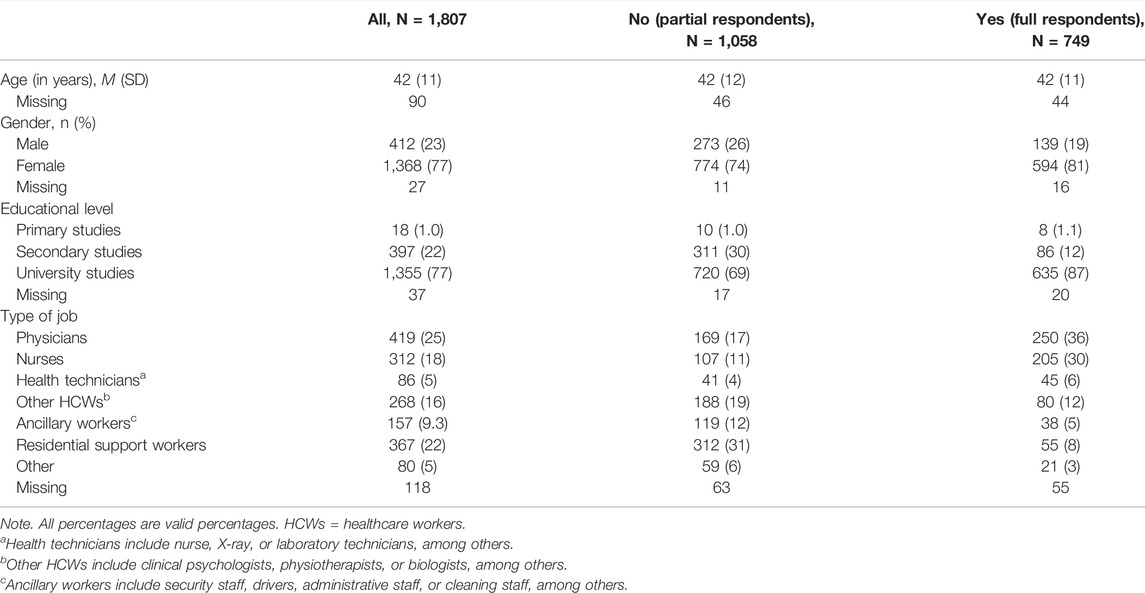
TABLE 1. Characteristics of the participants who underwent baseline assessment (full respondents) and who did not (partial respondents) as measured at follow-up [The COVID-19 HEalth caRe wOrkErS (HEROES) Study, Spain, 2021].
Overall, 56% of follow-up respondents screened positive for psychological distress, 21% for probable depression, and 51% for PTSD. Psychological distress, probable depression, and PTSD were more frequent among younger and female respondents, and respondents with higher educational levels—with substantial heterogeneity across specific job types (see Supplementary Table S3). Notably, follow-up mental health outcomes were comparable between full and partial respondents, with similar mean (SD) GHQ-12 score (3.9 [3.5] vs. 3.8 [3.4], respectively), mean (SD) PHQ-9 score (6.3 [5.1] vs. 6.4 [3.4], respectively), proportion of respondents screening positive for psychological distress (56% vs. 55%, respectively), and proportion of respondents screening positive for probable depression (21% vs. 21%, respectively).
Comparisons Between Baseline and Follow-Up Mental Health Outcomes
Comparisons between baseline and follow-up mental health outcomes among full respondents are shown in Table 2. The proportion of respondents screening positive for psychological distress and probable depression decreased, respectively, from 74% to 56% and from 28% to 21%. Figure 2 shows the distribution of trajectories of depression symptoms and psychological distress over time, overall and across baseline covariates. Trajectories show that, in terms of depression symptoms, 66% respondents remained asymptomatic/stable, 15% recovered, and 19% remained symptomatic or worsened over time. In terms of psychological distress, 18% respondents remained asymptomatic/stable, 26% recovered, and 56% remained symptomatic or worsened over time. The distribution of trajectories was heterogeneous across baseline covariates.
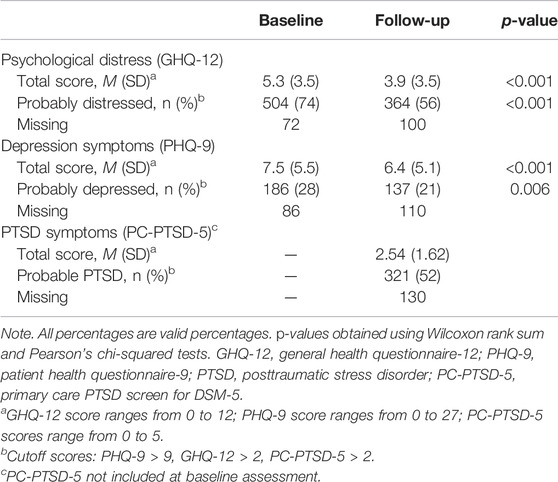
TABLE 2. Mental health outcomes among full respondents (N = 749) at baseline and follow-up [The COVID-19 HEalth caRe wOrkErS (HEROES) Study, Spain, 2021].
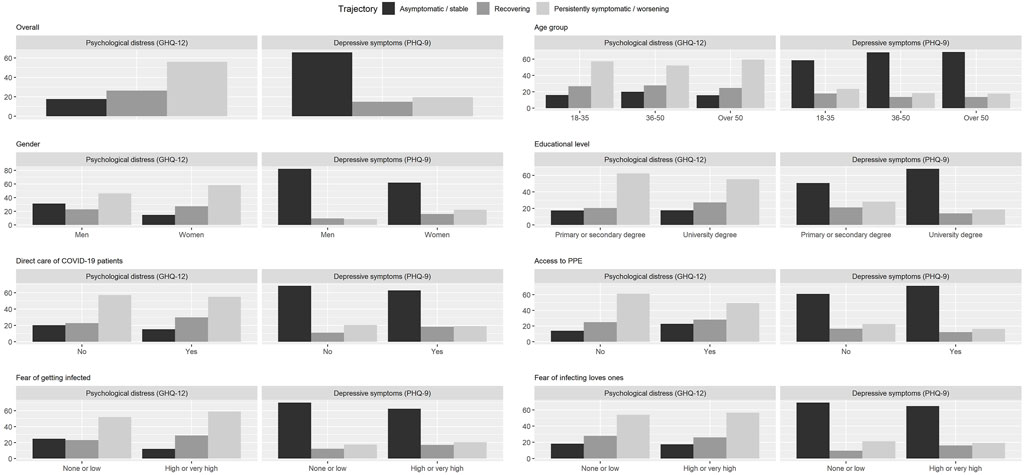
FIGURE 2. Mental health outcome trajectories of psychological distress and depression symptoms stratified by relevant variables. Trajectories include people with positive screening at baseline and negative screening at follow-up (recovering), people with positive or negative screening at baseline and positive screening at follow-up (persistently symptomatic/worsening) and people with negative screening at baseline and follow-up (asymptomatic stable) [The COVID-19 HEalth caRe wOrkErS (HEROES) Study, Spain, 2021].
Association Between Baseline Exposures and Follow-Up Mental Health Outcomes and Trajectories
Table 3 shows crude and adjusted estimates of the association between baseline exposures and follow-up mental health outcome scores among full respondents. Overall, women had higher scores (i.e., worse mental health) than men, and job-related factors such as direct involvement in the care of COVID-19, inadequate access to protective equipment, or fear of infecting oneself or loved ones were associated with higher negative mental health outcome scores–especially for PTSD, and with higher odds of testing positive for psychological distress, probable depression, and PTSD (see Supplementary Table S4). We repeated all models, first including further adjustment by baseline mental health outcome scores (see Supplementary Tables S5, S6) and then including Likert-type variables as dummy variables: results did not change.
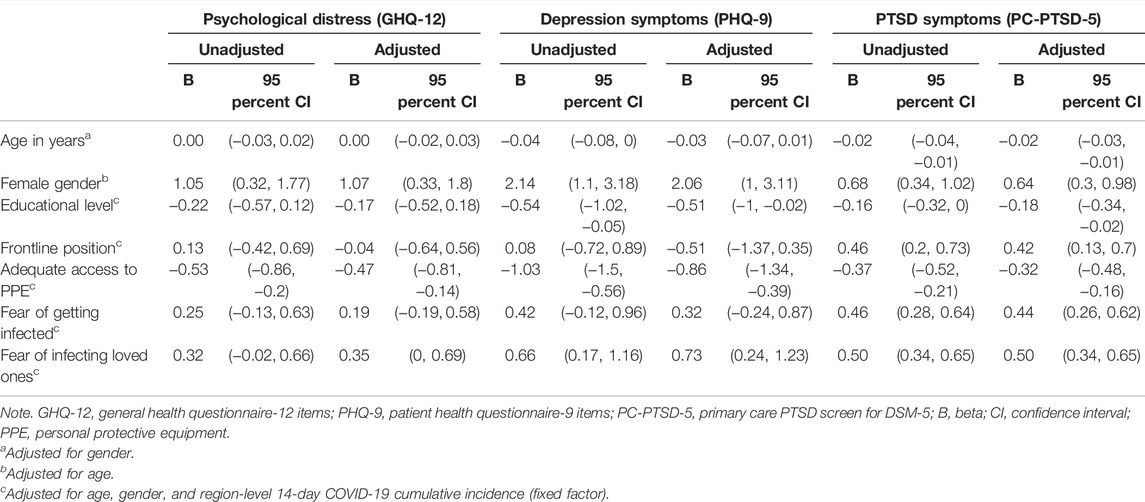
TABLE 3. Association between participants’ sociodemographic characteristics and COVID-19-related exposures, measured at baseline, and mental health outcomes’ total scores (psychological distress, depressive symptoms, and posttraumatic stress disorder symptoms), measured at follow-up (8 months) [The COVID-19 HEalth caRe wOrkErS (HEROES) Study, Spain, 2021].
Table 4 shows crude and adjusted associations between baseline exposures and trajectory membership for psychological distress and probable depression. Women showed higher symptom variability over time than men, as indicated by women’s higher odds of belonging to both the recovering and the persistently symptomatic/worsening categories for both psychological distress and probable depression. In terms of psychological distress, reporting inadequate access to personal protective equipment was associated with persistently symptomatic/worsening category membership. In terms of probable depression, fear of infecting loved ones was associated with recovering category membership. Results did not change in models including Likert-type variables as dummy variables.
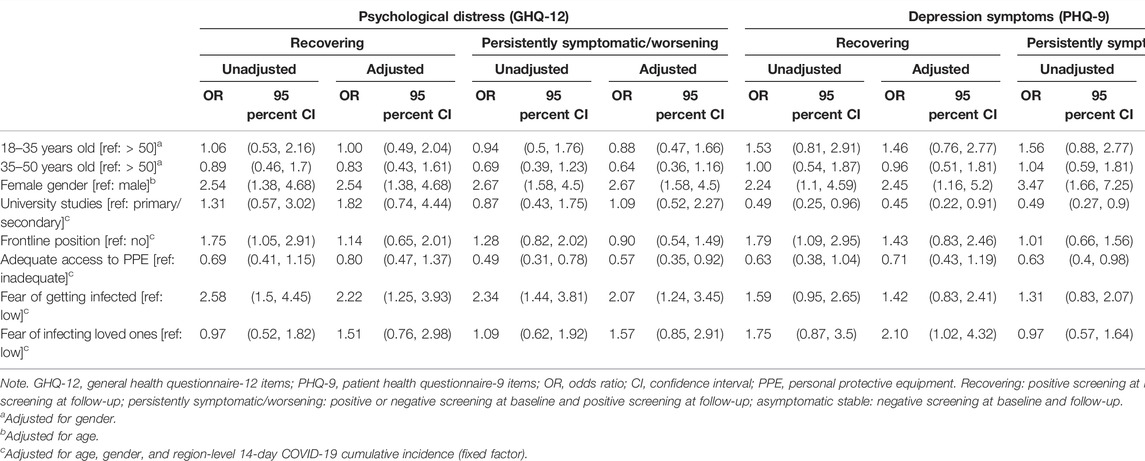
TABLE 4. Association between participants’ sociodemographic characteristics and COVID-19-related exposures, measured at baseline, and the probability of belonging to the trajectories recovering or persistently symptomatic/worsening (versus asymptomatic stable) at follow-up [The COVID-19 HEalth caRe wOrkErS (HEROES) Study, Spain, 2021].
Discussion
This study followed a cohort of HCWs from one of the earliest COVID-19 pandemic hotspots over the 1-year period after the initial pandemic outbreak. There was marked heterogeneity across individuals in terms of variation in mental health outcomes over time. While we detected general reductions in psychological distress (from 74% to 56%) and depression symptoms (from 28% to 21%), the overall burden of poor mental health among HCWs remained substantial 8 months after the pandemic onset (56% screened positive for psychological distress, 21% for probable depression, and 51% for PTSD). Our analysis of mental health outcome trajectories revealed that psychological distress and depression symptoms persisted or worsened over time for 56% and 19% of respondents, respectively. We identified prospective associations between certain baseline characteristics, such as being female, reporting inadequate access to personal protective equipment, or being afraid of getting infected and of infecting loved ones, and follow-up psychological distress, depression symptoms, and PTSD symptoms. These results highlight the importance of adapting, implementing, and scaling-up evidence-based public, occupational, and mental health interventions for HCWs to prevent their mental health from further deteriorating during the ongoing pandemic and its aftermath.
Early cross-sectional studies from high-incidence COVID-19 areas, such as the Chinese region of Wuhan [24], Italy [3, 5], or Spain [1], described the mental health toll taken by the pandemic on HCWs’ mental health, showing remarkable rates of psychological distress, anxiety, depression, and PTSD symptoms. In our study sample, estimates of the point prevalence of depression at baseline were similar than those found in Italy (25%) and Spain (28%), probably due to similar sample characteristics and study settings. Likewise, our baseline finding that three in four respondents were psychologically distressed is nearly identical to that of Lai et al. in Wuhan at the beginning of the pandemic (late January 2020). Additionally, a series of cross-sectional studies had already reported associations between HCWs’ characteristics, such as female gender, or inadequate access to personal protective equipment and negative mental health outcomes (i.e., anxiety or depression) [25–27]. Our study found these associations to persist within a prospective cohort design, lowering the risk of potential reverse causation bias and hence greatly enhancing interpretability for decision-making.
Other prospective studies have sought to describe the evolution of HCWs’ negative mental health outcomes over time using a variety of outcomes and follow-up periods [9–12, 27–30]. Somewhat in contrast to our results, López Steinmez and others reported a slight increase in psychological distress (from 40% to 46% point prevalence) between May and September, 2020, in a sample of 300 HCWs from Buenos Aires, Argentina. Differences in follow-up time probably accounts for this between-study difference, as they may have captured the early consequences of the initial pandemic outbreak while we conducted our assessments later, when renovated reasons for optimism (e.g., vaccine development and roll-out) had already started to emerge. Using a highly homogeneous sample of 200 nurses, Pinho and others reported stable trends in depression and decreasing trends in anxiety between April and November, 2020. Differences in sample composition make their results hardly comparable to our’s. Other studies have either used much shorter follow-up periods [27, 29, 30] or reported outcomes not comparable to our’s, such as insomnia [28] or job stress [12]. Our’s is the first prospective cohort analysis of risk factors for negative mental health outcomes among HCWs to adjust all associations of interest for potential confounding due to area-level COVID-19 cumulative incidence, in addition to adjustment for individual-level confounding. Notably, mounting evidence suggests higher rates of negative mental health outcomes among HCWs from regions with higher incidence [31].
To our knowledge, only one study has described the trajectories of mental health problems among HCWs during the COVID-19 pandemic [9]. Using latent class modelling based on scores on three mental health outcomes (depression, anxiety, and PTSD symptoms) between May and September, 2020, they found four distinct trajectories which are remarkably similar to ours in terms of interpretation and prevalence within the study sample: 19% respondents belonged to their “recovered” group (for 15% in our recovering group), 66% to their “resilient” group (for 66% in our asymptomatic stable group), and 7% and 8%, respectively, to their “sub-chronic” and “delayed” groups (for 19% in our symptomatic/worsening group). These same trajectories have been identified is studies using latent growth mixture modelling across many different populations that have experienced adversity [32]. Notably, this previous study did not assess psychological distress. Accordingly, our surprisingly high rates of persistence or worsening of psychological distress (56% of respondents) cannot be compared to other studies. While this result does not lend itself to easy interpretation until subsequent follow-up studies using the GHQ-12 emerge, it seems plausible that a substantial proportion of HCWs may potentially beneficiate from implementation of programs to lower psychological distress.
In addition to confirming associations previously reported in cross-sectional reports, our findings expand existing evidence in impactful ways for public health and clinical decision-making. First, by including a heterogeneous sample of HCWs with and without clinical duties, our study may serve to inform strategies aimed at non-clinical workers such as administrators or cleaners—largely overlooked in most studies examining mental health outcomes among HCWs during the COVID-19 pandemic. Second, our finding of scarce evidence of reliable baseline predictors of mental health outcome trajectories over time suggests that all HCWs should be offered easy-to-access mental health resources tailored to their needs (i.e., self-care and low-intensity psychotherapeutic interventions), regardless of profile in terms of sociodemographic characteristics and baseline clinical features.
Our study has limitations. First, we used a non-random sample that increases probability of some degree of collider bias and hinders transportability of study results across settings. Also, and in line with other multi-center studies [1, 4], response rates varied significantly across sites and facilities, and the possibility of self-selection bias cannot be ruled out. Nevertheless, the baseline sociodemographic characteristics and mental health outcomes were however similar to another Spanish study with a larger and somewhat more representative sample of HCWs [1] and to other, similar European studies [2, 3]. Second, because of the use of observational data, effect estimates are potentially subject to some degree of residual confounding. Notably, substantial residual confounding is unlikely given that we included measures on all major individual- and region-level confounders and that estimates from crude and adjusted associations are roughly similar. Moreover, sensitivity analyses exploring differences between subsamples (e.g., full vs. partial respondents) and adjusting for baseline measurements of mental health outcomes obtained similar results, suggesting that our models were robust to different model specifications. Third, two thirds of baseline respondents were lost to follow-up. Dropout was independent from age, gender, and mental health outcomes at baseline, but people lost to follow were slightly more concerned about getting the virus and infecting their loved ones (data not shown). Fourth, limitations of self-reports for diagnostic screening are widely known [33]. In the context of HCWs’ reactions to an initial pandemic outbreak, available diagnostic thresholds might have misclassified early, adaptive reactions to acute stressors as probable disorders (i.e., false positives). Notwithstanding, we used widely accepted screening instruments with good psychometric properties validated worldwide. Last, we calculated outcome trajectories based on information from two time points only. Future steps will include ascertainment of mental health outcomes in subsequent follow-up assessments and adoption of data-driven latent growth modelling approaches in addition to previously established categories based on clinical implications.
This is the first study to describe the trajectories of change of a large sample of HCWs from an early pandemic hotspot over a long follow-up period. Our results suggest preventative and restorative strategies at various levels (i.e., public, occupational, and specialized mental health), and outlines modifiable factors that might inform resource allocation, such as provision of protective equipment or being in direct care of COVID-19 patients. Further studies exploring the long-term impact of the pandemic among HCWs are warranted.
Ethics Statement
The studies involving human participants were reviewed and approved by the Ethics Review Board at the Hospital Universitario La Paz. The patients/participants provided their written informed consent to participate in this study.
Author Contributions
RM: conceptualization, methodology, software, formal analysis, investigation, resources, data curation, writing—original draft, visualization, and funding acquisition. EF-J, IM-S, and BM-K: investigation, resources, writing—review and editing, project administration, and funding acquisition. IM-M and FM: investigation, resources, writing—review and editing, and project administration. FJ and JA-J, and SM: investigation, resources, and project administration. JA-M: writing—review and editing and funding acquisition. RB: writing—review and editing. M-FB-O: conceptualization, supervision, and funding acquisition. GM-A: conceptualization, methodology, validation, investigation, resources, writing—original draft, supervision, and funding acquisition.
Funding
This work was supported by the Instituto de Salud Carlos III (ISCIII) and co-funded by the European Union (grant numbers: COV20/00988 and PI17/00768), the European Union's Horizon 2020 research and innovation programme Societal Challenges (grant number: 101016127), and the Fundación Española de Psiquiatría y Salud Mental.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.ssph-journal.org/articles/10.3389/ijph.2022.1604553/full#supplementary-material
References
1. Alonso, J, Vilagut, G, Mortier, P, Ferrer, M, Alayo, I, Aragón-Peña, A, et al. Mental Health Impact of the First Wave of COVID-19 Pandemic on Spanish Healthcare Workers: A Large Cross-Sectional Survey. Revista de Psiquiatría y Salud Ment (2021) 14(2):90–105. doi:10.1016/j.rpsm.2020.12.001
2. Azoulay, E, Cariou, A, Bruneel, F, Demoule, A, Kouatchet, A, Reuter, D, et al. Symptoms of Anxiety, Depression, and Peritraumatic Dissociation in Critical Care Clinicians Managing Patients with COVID-19. A Cross-Sectional Study. Am J Respir Crit Care Med (2020) 202(10):1388–98. doi:10.1164/rccm.202006-2568oc
3. Lasalvia, A, Bonetto, C, Porru, S, Carta, A, Tardivo, S, Bovo, C, et al. Psychological Impact of COVID-19 Pandemic on Healthcare Workers in a Highly Burdened Area of north-east Italy. Epidemiol Psychiatr Sci (2021) 30:e1. doi:10.1017/S2045796020001158
4. Morawa, E, Schug, C, Geiser, F, Beschoner, P, Jerg-Bretzke, L, Albus, C, et al. Psychosocial burden and Working Conditions during the COVID-19 Pandemic in Germany: The VOICE Survey Among 3678 Health Care Workers in Hospitals. J Psychosomatic Res (2021) 144:110415. doi:10.1016/j.jpsychores.2021.110415
5. Rossi, R, Socci, V, Pacitti, F, Di Lorenzo, G, Di Marco, A, Siracusano, A, et al. Mental Health Outcomes Among Frontline and Second-Line Health Care Workers during the Coronavirus Disease 2019 (COVID-19) Pandemic in Italy. JAMA Netw Open (2020) 3(5):e2010185. doi:10.1001/jamanetworkopen.2020.10185
6. Santabárbara, J, Bueno-Notivol, J, Lipnicki, DM, Olaya, B, Pérez-Moreno, M, Gracia-García, P, et al. Prevalence of Anxiety in Health Care Professionals during the COVID-19 Pandemic: A Rapid Systematic Review (On Published Articles in Medline) with Meta-Analysis. Prog Neuro-Psychopharmacology Biol Psychiatry (2021) 107:110244. doi:10.1016/j.pnpbp.2021.110244
7. Wanigasooriya, K, Palimar, P, Naumann, DN, Ismail, K, Fellows, JL, Logan, P, et al. Mental health symptoms in a cohort of hospital healthcare workers following the first peak of the COVID-19 pandemic in the UK. BJPsych Open (2021) 7:e24. doi:10.1192/bjo.2020.150
8. Ayuso-Mateos, JL, Mediavilla, R, Rodriguez, KR, and Bravo, MF. Informing the Response to COVID-19 in Spain: Priorities for Mental Health Research. Revista de Psiquiatría y Salud Ment (English Edition) (2021) 14(2):79–82. doi:10.1016/j.rpsmen.2021.04.001
9. Dufour, MM, Bergeron, N, Rabasa, A, Guay, S, and Geoffrion, S. Assessment of Psychological Distress in Health-care Workers during and after the First Wave of COVID-19: A Canadian Longitudinal Study: Évaluation de la Détresse Psychologique Chez Les Travailleurs de la Santé Durant et Après la Première Vague de la COVID-19: une étude longitudinale canadienne. Can J Psychiatry (2021) 66:807–14. doi:10.1177/07067437211025217
10. López Steinmetz, LC, Herrera, CR, Fong, SB, and Godoy, JC. A Longitudinal Study on the Changes in Mental Health of Healthcare Workers during the COVID-19 Pandemic. Psychiatry (2021) 30:1–16. doi:10.1080/00332747.2021
11. Pinho, L, Correia, T, Sampaio, F, Sequeira, C, Teixeira, L, Lopes, M, et al. The Use of Mental Health Promotion Strategies by Nurses to Reduce Anxiety, Stress, and Depression during the COVID-19 Outbreak: A Prospective Cohort Study. Environ Res (2021) 195:110828. doi:10.1016/j.envres.2021.110828
12. Sasaki, N, Asaoka, H, Kuroda, R, Tsuno, K, Imamura, K, and Kawakami, N. Sustained Poor Mental Health Among Healthcare Workers in COVID-19 Pandemic: A Longitudinal Analysis of the Four-Wave Panel Survey over 8 Months in Japan. J Occup Health Enero de (2021) 63(1):e12227. doi:10.1002/1348-9585.12227
13. Mascayano, F, van der Ven, E, Moro, MF, Schilling, S, Alarcón, S, Al Barathie, J, et al. The Impact of the COVID-19 Pandemic on the Mental Health of Healthcare Workers: Study Protocol for the COVID-19 HEalth caRe wOrkErS (HEROES) Study. Soc Psychiatry Psychiatr Epidemiol (2022) 57:633–45. doi:10.1007/s00127-021-02211-9
14. Mediavilla, R, Fernández-Jiménez, E, Martínez-Alés, G, Moreno-Küstner, B, Martinez-Morata, I, Jaramillo, F, et al. Role of Access to Personal Protective Equipment, Treatment Prioritization Decisions, and Changes in Job Functions on Health Workers’ Mental Health Outcomes during the Initial Outbreak of the COVID-19 Pandemic. J Affective Disord (2021) 295:405–9. doi:10.1016/j.jad.2021.08.059
15. Sánchez-López, MP, and Dresch, V. The 12-item General Health Questionnaire (Ghq-12): Reliability, External Validity and Factor Structure in the Spanish Population. Psicothema (2008) 20(4):839–43.
16. Diez-Quevedo, C, Rangil, T, Sanchez-Planell, L, Kroenke, K, and Spitzer, RL. Validation and Utility of the Patient Health Questionnaire in Diagnosing Mental Disorders in 1003 General Hospital Spanish Inpatients. Psychosomatic Med (2001) 63(4):679–86. doi:10.1097/00006842-200107000-00021
17. Domínguez-Salas, S, Gómez-Salgado, J, Andrés-Villas, M, Díaz-Milanés, D, Romero-Martín, M, and Ruiz-Frutos, C. Psycho-Emotional Approach to the Psychological Distress Related to the COVID-19 Pandemic in Spain: A Cross-Sectional Observational Study. Healthcare (2020) 8(3):190. doi:10.3390/healthcare8030190
18. Goldberg, DP, Gater, R, Sartorius, N, Ustun, TB, Piccinelli, M, Gureje, O, et al. The Validity of Two Versions of the GHQ in the WHO Study of Mental Illness in General Health Care. Psychol Med (1997) 27(1):191–7. doi:10.1017/s0033291796004242
19. Manea, L, Gilbody, S, and McMillan, D. Optimal Cut-Off Score for Diagnosing Depression with the Patient Health Questionnaire (PHQ-9): a Meta-Analysis. Cmaj (2012) 184(3):E191–E196. doi:10.1503/cmaj.110829
20. Prins, A, Bovin, MJ, Smolenski, DJ, Marx, BP, Kimerling, R, Jenkins-Guarnieri, MA, et al. The Primary Care PTSD Screen for DSM-5 (PC-PTSD-5): Development and Evaluation within a Veteran Primary Care Sample. J Gen Intern Med (2016) 31(10):1206–11. doi:10.1007/s11606-016-3703-5
21. Ouimette, P, Wade, M, Prins, A, and Schohn, M. Identifying PTSD in Primary Care: Comparison of the Primary Care-PTSD Screen (PC-PTSD) and the General Health Questionnaire-12 (GHQ). J Anxiety Disord (2008) 22(2):337–43. doi:10.1016/j.janxdis.2007.02.010
22. Pearl, J. [Bayesian Analysis in Expert Systems]: Comment: Graphical Models, Causality and Intervention. Stat Sci (1993) 8(3):266–9. doi:10.1214/ss/1177010894
23. Norman, G. Likert Scales, Levels of Measurement and the “Laws” of Statistics. Adv Health Sci Educ (2010) 15(5):625–32. doi:10.1007/s10459-010-9222-y
24. Lai, J, Ma, S, Wang, Y, Cai, Z, Hu, J, Wei, N, et al. Factors Associated with Mental Health Outcomes Among Health Care Workers Exposed to Coronavirus Disease 2019. JAMA Netw Open (2020) 3(3):e203976. doi:10.1001/jamanetworkopen.2020.3976
25. Rodriguez-Menéndez, G, Rubio-García, A, Conde-Alvarez, P, Armesto-Luque, L, Garrido-Torres, N, Capitan, L, et al. Short-term Emotional Impact of COVID-19 Pandemic on Spaniard Health Workers. J Affective Disord (2021) 278:390–4. doi:10.1016/j.jad.2020.09.079
26. Pappa, S, Ntella, V, Giannakas, T, Giannakoulis, VG, Papoutsi, E, and Katsaounou, P. Prevalence of Depression, Anxiety, and Insomnia Among Healthcare Workers during the COVID-19 Pandemic: A Systematic Review and Meta-Analysis. Brain Behav Immunity1 de agosto de (2020) 88:901–7. doi:10.1016/j.bbi.2020.05.026
27. Sampaio, F, Sequeira, C, and Teixeira, L. Impact of COVID-19 Outbreak on Nurses' Mental Health: A Prospective Cohort Study. Environ Res (2021) 194:110620. doi:10.1016/j.envres.2020.110620
28. Abdalla, M, Chiuzan, C, Shang, Y, Ko, G, Diaz, F, Shaw, K, et al. Factors Associated with Insomnia Symptoms in a Longitudinal Study Among New York City Healthcare Workers during the COVID-19 Pandemic. Ijerph (2021) 18(17):8970. doi:10.3390/ijerph18178970
29. Van Steenkiste, E, Schoofs, J, Gilis, S, and Messiaen, P. Mental Health Impact of COVID-19 in Frontline Healthcare Workers in a Belgian Tertiary Care Hospital: a Prospective Longitudinal Study. Acta Clin Belg (2021) 28:1–8.
30. Zhou, Y, Ding, H, Zhang, Y, Zhang, B, Guo, Y, Cheung, T, et al. Prevalence of Poor Psychiatric Status and Sleep Quality Among Frontline Healthcare Workers during and after the COVID-19 Outbreak: a Longitudinal Study. Transl Psychiatry (2021) 11(1):223. doi:10.1038/s41398-020-01190-w
31. Romero, CS, Delgado, C, Catalá, J, Ferrer, C, Errando, C, Iftimi, A, et al. COVID-19 Psychological Impact in 3109 Healthcare Workers in Spain: The PSIMCOV Group. Psychol Med (2020) 14. 1–7. doi:10.1017/S0033291720001671
32. Galatzer-Levy, IR, Huang, SH, and Bonanno, GA. Trajectories of Resilience and Dysfunction Following Potential Trauma: A Review and Statistical Evaluation. Clin Psychol Rev (2018) 63:41–55. doi:10.1016/j.cpr.2018.05.008
Keywords: anxiety, mental health, healthcare workers, COVID-19, depression, prospective cohort
Citation: Mediavilla R, Fernández-Jiménez E, Martinez-Morata I, Jaramillo F, Andreo-Jover J, Morán-Sánchez I, Mascayano F, Moreno-Küstner B, Minué S, Ayuso-Mateos JL, Bryant RA, Bravo-Ortiz M-F and Martínez-Alés G (2022) Sustained Negative Mental Health Outcomes Among Healthcare Workers Over the First Year of the COVID-19 Pandemic: A Prospective Cohort Study. Int J Public Health 67:1604553. doi: 10.3389/ijph.2022.1604553
Received: 26 October 2021; Accepted: 31 May 2022;
Published: 17 June 2022.
Edited by:
Olaf von dem Knesebeck, University Medical Center Hamburg-Eppendorf, GermanyReviewed by:
Bijit Biswas, India Institute of Medical Sciences Gorakhpur, IndiaCopyright © 2022 Mediavilla, Fernández-Jiménez, Martinez-Morata, Jaramillo, Andreo-Jover, Morán-Sánchez, Mascayano, Moreno-Küstner, Minué, Ayuso-Mateos, Bryant, Bravo-Ortiz and Martínez-Alés. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Roberto Mediavilla, cm9iZXJ0by5tZWRpYXZpbGxhQHVhbS5lcw==
This Original Article is part of the IJPH Special Issue “The Impact of the COVID-19 Pandemic on Mental Health”