Abstract
Objectives: Dengue Fever (DF) is an arboviral disease caused by the Dengue virus (DENV). This study aims to assess the association of dengue prevalence with patients’ residential areas and hematological laboratory findings (Total platelet count, immunoglobulins, and dengue antigens) during COVID-19 pandemic.
Methods: A retrospective study was conducted at the Emergency department of Jinnah Postgraduate Medical Center, Karachi from October to December 2021. All the patients irrespective of their ages presenting to the ED with either of the following complaints: fever; GIT problems; vomiting; body ache; bleeding were included in our study.
Results: Our study comprised 189 patients in total in which the females (n = 172) outnumbered the males (n = 17). Out of all, 84.7% of the patients were febrile having a low-grade fever on average. Korangi district had the most dengue cases, while Keamari had the fewest. There was no significant association reported between mean platelet count, mean TLC, and mean hemoglobin levels with dengue positivity.
Conclusion: There is a concerning rise in DF cases in Karachi, particularly in the Korangi district. Despite the COVID-19 pandemic, DF demands urgent attention.
Introduction
Dengue Fever (DF) is an arboviral disease caused by the Dengue virus (DENV), and it is a serious public health problem owing to its rapid spread. The most prevalent mosquito vectors for the transmission of the infection are Aedes aegypti and Aedes albopictus [1]. According to a report, DF is estimated to affect 3.9 billion people worldwide and out of which 70% burden exists in Asia [2]. Countries that are worst affected by the DENV are Pakistan, Bangladesh, India, and Sri Lanka [3]. Pakistan is endemic to the DENV for the last 30 years [4]. The first incidence of DF in Pakistan was recorded in Karachi in 1994 [5]. Between 2015 and 2019, there were 90,400 dengue cases and 169 fatalities in Pakistan [4]. Similarly, 3,442 confirmed dengue cases had been reported in 2020 [6]. According to the news, a substantial increase in dengue infections was recorded in the latter 3 months of 2021, with 48,906 cases reported as of November 25, 2021, with 183 fatalities [7, 8].
DF is a single disease that can manifest in a variety of ways, from asymptomatic seroconversion to moderate or severe DF, which can result in shock, severe bleeding, and even death [9, 10]. Dengue hemorrhagic fever (DHF) and Dengue shock syndrome (DSS) are the two most common clinical complications caused by DF. DHF and DSS are reversible vascular complications of DF that cause severe thrombocytopenia and increased vascular permeability [11]. For this reason, a decrease in platelet and white blood cell counts, as well as an increase in plasma leakage, are regarded as highly efficient indicators of dengue infection [12]. Dengue infection symptoms include vomiting, body aches, abdominal pain, and bleeding, in addition to a high temperature [13].
Pakistan is already dealing with the COVID-19 pandemic and another dengue outbreak would be disastrous for the country’s already debilitated healthcare infrastructure. Moreover, since DF and COVID-19 have similar clinical symptoms, they can readily exist as co-infection [14]. For this reason, it is important to have fore-hand preparation of the healthcare system as well as the authorities to avoid further harm and damage.
This study aims to assess the profile of dengue patients presenting to the Emergency Department (ED) of a tertiary care hospital during COVID-19 pandemic. It includes determining their sociodemographic factors including the patients’ residential area to determine dengue endemic regions of Karachi, and the hematological laboratory findings including total platelet count, immunoglobulin M (IgM), immunoglobulin G (IgG), and non-structural protein 1 (NS1) antigens with the associated symptoms of DF.
Methods
Design and Setting
A retrospective study was conducted at the ED of Jinnah Postgraduate Medical Center (JPMC) from October to December 2021. JPMC is a tertiary care public hospital located in Karachi, Pakistan. The ethical approval of the study was obtained from the hospital’s Institutional Review Board (IRB) (NO.F.281/2022-GENL/242/JPMC).
Inclusion Criteria
All the patients irrespective of their ages presenting to the ED with either of the following complaints: fever; GIT problems; vomiting; body ache; bleeding were included in our study. Patients who did not give consent or had chronic diseases or gave incomplete information were excluded from our study. We only included the patients who met the inclusion criteria.
Data Collection
The data were collected from the ED of JPMC. It included patients’ demographical details (age, gender, and residential area), presenting complaints, lab tests, temperature, and dengue test reports. Dengue infection were confirmed through standard Dengue NS1 antigen enzyme-linked immunosorbent assay (ELISA) and standard Dengue IgM or IgG Capture ELISA kits (Standard Diagnostics Inc, Kyonggi-do Korea). Patient’s identities, personal information, and reports were kept confidential and only the primary investigators were given access to that data. All the ethical considerations were kept in mind throughout the study.
Statistical Analysis
IBM Corp. Released 2016. IBM SPSS Statistics for Windows, Version 24.0. Armonk, NY: IBM Corp. was used to perform the data analysis. The analysis was performed in four stages. First, the frequencies of all the variables were determined. Then, mean ± standard deviation (SD) values of age, temperature, hemoglobin levels, total leukocyte count (TLC), and platelet count were calculated using descriptive statistics. To evaluate the association between categorical variables, we performed Pearson’s chi-squared tests. Lastly, we performed the Independent Samples T-test to determine the relationship between categorical and continuous variables. A p-value of <0.05 was considered significant, statistically.
Results
Demographical and Baseline Characteristics of the Patients
Our study comprised 189 patients in total in which the females (n = 172) outnumbered the males (n = 17) as depicted by the pie chart in Figure 1. The mean age of the participants was reported to be 31.59 ± 14.68 years. The participants were reported to have a low fever on average. Average platelet count and other hematological parameters are mentioned in Table 1. Upon district-wise distribution of the participants, more than one-third of them (36%) were the residents of Korangi district. The second and third most common districts were Karachi East (23%) and Malir (14%), respectively. They were followed by Karachi Central, Karachi South, areas outside Karachi, Karachi West, and Keamari (Figure 2).
FIGURE 1
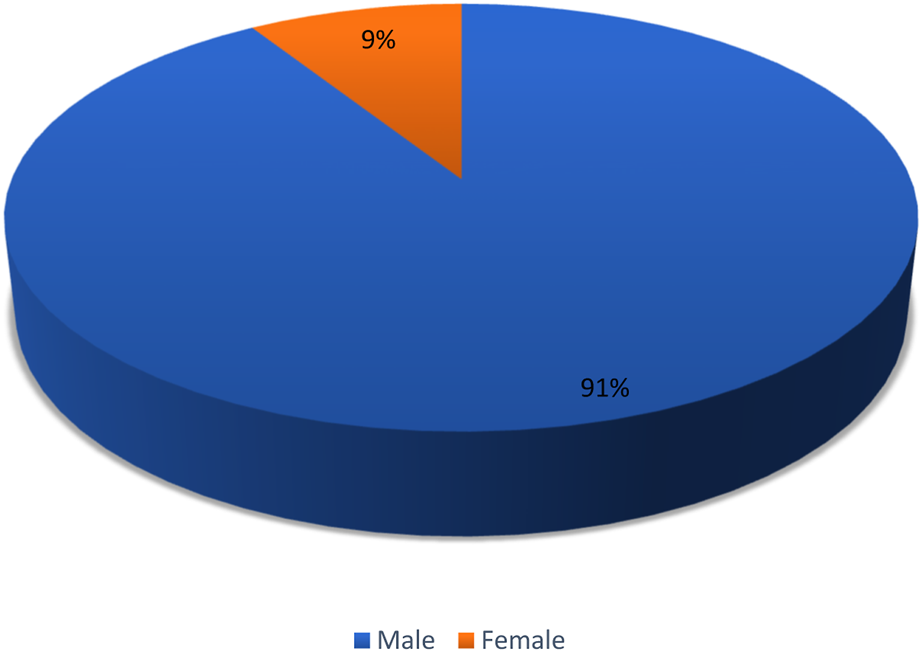
Gender-based distribution of the patients (Karachi, Pakistan. 2021).
TABLE 1
| Participants’ characteristics | Mean ± SD |
|---|---|
| Age (years) | 31.59 ± 14.68 |
| Temperature (°F) | 100.59 ± 1.61 |
| Platelet count (mcL) | 108217.99 ± 152660.41 |
| Hemoglobin level (g/dL) | 13.20 ± 2.51 |
| Total leukocyte count (cell/ccm) | 5.18 ± 2.87 |
Means of ages, body temperature, and hematological parameters of patients (Karachi, Pakistan. 2021).
FIGURE 2
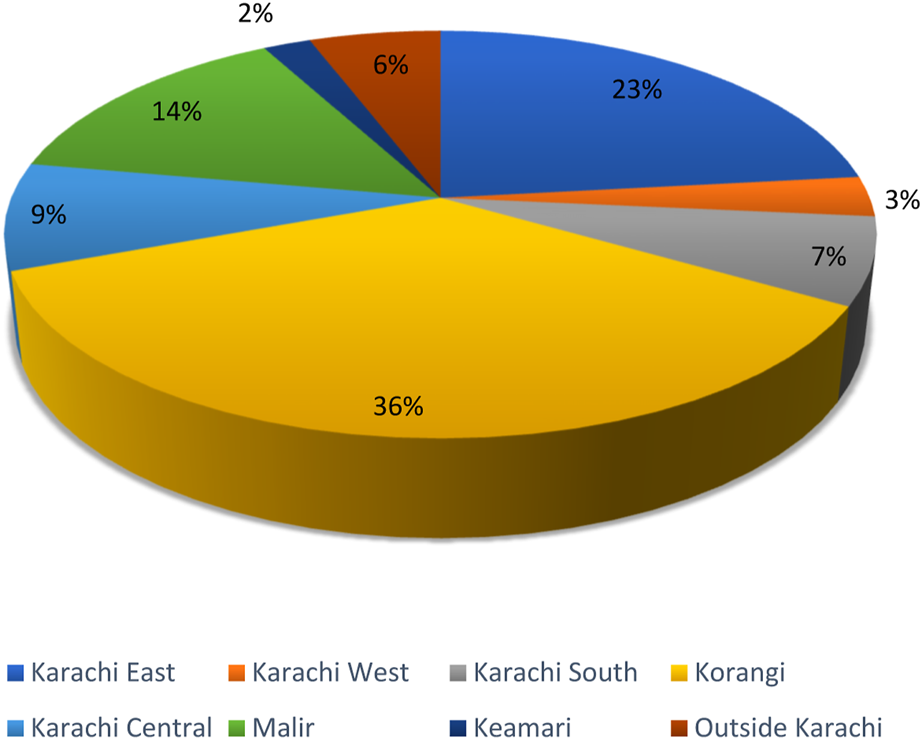
District-wise distribution of the patients (Karachi, Pakistan. 2021).
Dengue Diagnosis
The diagnosis of the DENV was made on the basis of different antigens’ serum positivity and negativity. Out of 159 patients who were positive for DENV, around three-quarters of them (73.5%) were positive for NS1 antigen, while a few (2.6%, 5.3%) were positive for IgM and IgG respectively. The remaining ones (2.6%) were positive for both IgM and IgG (Table 2).
TABLE 2
| Antigen | Subgroup | No. of participants (%) |
|---|---|---|
| NS1 | Positive | 139 (73.5) |
| Negative | 28 (14.8) | |
| IgM | Positive | 5 (2.6) |
| Negative | — | |
| IgG | Positive | 10 (5.3) |
| Negative | 1 (0.5) | |
| IgG/IgM | Positive | 5 (2.6) |
| Negative | 1 (0.5) |
Antigen-wise division of dengue diagnosis (Karachi, Pakistan. 2021).
Signs and Symptoms
Upon arrival at the hospital, the participants were checked for their dengue status. A substantial number of subjects (84.1%) tested positive for the DENV. Out of all, 84.7% of the patients were febrile having a low-grade fever on average. A huge majority (>90%) of the patients did not have the following signs and symptoms: headache; vertigo; rash; rigors; chills; fits; gallbladder wall (GBW) thickening; nausea; altered level of consciousness (ALOC); hematuria; per rectal bleeding; oral bleeding; epistaxis; generalized body weakness; diarrhea; shortness of breath (SOB); cough; epigastric pain; hematemesis. Nonetheless, generalized body ache (31.7%), abdominal pain (14.8%), and vomiting (29.6%) were more prevalent amongst the patients in comparison with other symptoms (Table 3).
TABLE 3
| Signs/symptoms | Subgroup | No. of participants (%) |
|---|---|---|
| Dengue status | Positive | 159 (84.1) |
| Negative | 30 (15.9) | |
| Fever status | Febrile | 160 (84.7) |
| Afebrile | 29 (15.3) | |
| Headache | Yes | 6 (3.2) |
| No | 183 (96.8) | |
| Vertigo | Yes | 2 (1.1) |
| No | 187 (98.9) | |
| Rash | Yes | 4 (2.1) |
| No | 185 (97.9) | |
| Rigors | Yes | 2 (1.1) |
| No | 187 (98.9) | |
| Chills | Yes | 10 (5.3) |
| No | 179 (94.7) | |
| Fits | Yes | 2 (1.1) |
| No | 187 (98.9) | |
| Gall bladder wall thickening | Yes | 6 (3.2) |
| No | 183 (96.8) | |
| Nausea | Yes | 13 (6.9) |
| No | 176 (93.1) | |
| Altered level of consciousness | Yes | 3 (1.6) |
| No | 186 (98.4) | |
| Hematuria | Yes | 2 (1.1) |
| No | 187 (98.9) | |
| Per rectal bleeding | Yes | 3 (1.6) |
| No | 186 (98.4) | |
| Oral bleeding | Yes | 7 (3.7) |
| No | 182 (96.3) | |
| Epistaxis | Yes | 13 (6.9) |
| No | 176 (93.1) | |
| Generalized body weakness | Yes | 8 (4.2) |
| No | 181 (95.8) | |
| Diarrhea | Yes | 14 (7.4) |
| No | 175 (92.6) | |
| Shortness of breath | Yes | 5 (2.6) |
| No | 184 (97.4) | |
| Cough | Yes | 3 (1.6) |
| No | 186 (98.4) | |
| Generalized body ache | Yes | 60 (31.7) |
| No | 129 (68.3) | |
| Abdominal pain | Yes | 28 (14.8) |
| No | 161 (85.2) | |
| Epigastric pain | Yes | 6 (3.2) |
| No | 183 (96.8) | |
| Vomiting | Yes | 56 (29.6) |
| No | 133 (70.4) | |
| Hematemesis | Yes | 7 (3.7) |
| No | 182 (96.3) |
Signs and symptoms in patients (Karachi, Pakistan. 2021).
Association of Dengue With Categorical and Continuous Variables
Our study reported a significant association between the patients’ district of residence and dengue status with Korangi having the greatest number of dengue cases (n = 62) and Keamari having the least ones (n = 3) (p = 0.053). According to our study, symptoms of vertigo and vomiting were significantly lower in dengue positive patients (p = 0.024; p = 0.010). Nevertheless, our study reported no significant association between dengue positivity and the following signs and symptoms: headache; rash; rigors; chills; fits; GBW thickening; nausea; ALOC; hematuria; per rectal bleeding; oral bleeding; epistaxis; generalized body weakness; diarrhea; SOB; cough; generalized body ache; abdominal pain; epigastric pain; hematemesis. Moreover, there was no significant gender difference reported (Table 4). There was no significant association reported between mean platelet count, mean TLC, and mean hemoglobin levels with dengue positivity (Table 5).
TABLE 4
| Variable | Subgroup | No. of participants investigated | No. of participants positive for DF | p-value |
|---|---|---|---|---|
| Gender | Male | 61 | 55 | 0.117 |
| Female | 128 | 104 | ||
| District | Karachi East | 44 | 35 | 0.053 |
| Karachi West | 6 | 6 | ||
| Karachi South | 13 | 8 | ||
| Karachi Central | 16 | 11 | ||
| Korangi | 68 | 62 | ||
| Malir | 27 | 25 | ||
| Kemari | 4 | 3 | ||
| Outside Karachi | 11 | 9 | ||
| Fever status | Febrile | 160 | 134 | 1.000 |
| Afebrile | 29 | 25 | ||
| Headache | Yes | 6 | 6 | 0.592 |
| No | 183 | 153 | ||
| Vertigo | Yes | 2 | 0 | 0.024 |
| No | 187 | 159 | ||
| Rash | Yes | 4 | 2 | 0.119 |
| No | 185 | 157 | ||
| Rigors | Yes | 2 | 2 | 1.000 |
| No | 187 | 157 | ||
| Chills | Yes | 10 | 8 | 0.661 |
| No | 179 | 151 | ||
| Fits | Yes | 2 | 1 | 0.293 |
| No | 187 | 158 | ||
| Gall bladder wall thickening | Yes | 6 | 4 | 0.243 |
| No | 183 | 155 | ||
| Nausea | Yes | 13 | 13 | 0.228 |
| No | 176 | 146 | ||
| Altered level of consciousness | Yes | 3 | 2 | 0.406 |
| No | 186 | 157 | ||
| Hematuria | Yes | 2 | 2 | 1.000 |
| No | 187 | 157 | ||
| Per rectal bleeding | Yes | 3 | 3 | 1.000 |
| No | 186 | 156 | ||
| Oral bleeding | Yes | 7 | 6 | 1.000 |
| No | 182 | 153 | ||
| Epistaxis | Yes | 13 | 12 | 0.696 |
| No | 176 | 147 | ||
| Generalized body weakness | Yes | 8 | 7 | 1.000 |
| No | 181 | 152 | ||
| Diarrhea | Yes | 14 | 10 | 0.244 |
| No | 175 | 149 | ||
| Shortness of breath | Yes | 5 | 3 | 0.179 |
| No | 184 | 156 | ||
| Cough | Yes | 3 | 3 | 1.000 |
| No | 186 | 156 | ||
| Generalized body ache | Yes | 60 | 50 | 0.839 |
| No | 129 | 109 | ||
| Abdominal pain | Yes | 28 | 24 | 1.000 |
| No | 161 | 135 | ||
| Epigastric pain | Yes | 6 | 5 | 1.000 |
| No | 183 | 154 | ||
| Vomiting | Yes | 56 | 53 | 0.010 |
| No | 133 | 106 | ||
| Hematemesis | Yes | 7 | 7 | 0.599 |
| No | 182 | 152 |
Association of dengue positivity with gender, district, and signs/symptoms of patients (Karachi, Pakistan. 2021).
TABLE 5
| Hematological marker | Dengue | Mean difference | p-value | |
|---|---|---|---|---|
| Positive | Negative | |||
| Mean platelet count ± SD | 107862.89 ± 149369.32 | 110100.00 ± 171814.12 | 2237.11 | 0.942 |
| Mean total leukocyte count ± SD | 5.04 ± 2.84 | 6.44 ± 3.15 | 1.39 | 0.307 |
| Mean hemoglobin level ± SD | 13.13 ± 2.49 | 16.00 ± 0.00 | 2.87 | 0.264 |
Association of dengue positivity with hematological parameters of patients (Karachi, Pakistan. 2021).
Discussion
In this retrospective study, the profile of dengue patients has been assessed whilst COVID-19 was still in effect. In low- and middle-income nations like Pakistan, the co-occurrence of these two infectious diseases might have a significant adverse effect on both the population and the economy [15].
Dengue infections were confirmed through antigen and antibody detection. Several patients tested positive for NS1 antigen but relatively few tested positive for IgG and IgM antibodies. This result shows that the NS1 antigen test was a more potent diagnostic technique for the identification of DF as compared to dengue IgM and IgG antibodies detection.
In contrast to other common symptoms of DF, individuals were more likely to have generalized body ache, abdominal pain, and vomiting. This result was in accordance with a study conducted in Karachi [16].
Additionally, the area of residence of each participant was also included, and it was separated into the districts of Karachi. This was done to determine where the majority of cases originated, which will assist in identifying dengue endemic locations. The results indicated that most of the cases originated in the Korangi district, followed by Karachi East and Malir district. With a population density of 3,900 people per square kilometer (10,000/sq mi), Karachi is an extremely populated city [17]. The two primary causes of the rise of dengue virus infection in tropical emerging nations are an unpredicted rise in population and unplanned urban expansion that leads to major public health problems [18].
This study of patients with dengue showed that the issue of DF has grown even more serious as authorities are busy dealing with COVID-19. Our study concluded that Korangi district was determined to be the most significant dengue-endemic area in Karachi. It is important that the general population, and especially healthcare professionals, should be aware of preventive techniques since doing so will help in the efficient diagnosis that allows appropriate patient care, generation of accurate epidemiological data, and implementation of effective public health actions.
This study shows that there were more female targets than male targets among the affected patients. This is in contrast to many researches where the majority of the patients were male [19, 20]. Social, cultural, and environmental factors may have led to the phenomena of gender specificity in relation to dengue infection. This could be due to society’s neglect towards women’s health problems along with amenia and their debilitating immune system [21].
The district-wise distribution of dengue patients in this study makes it one of its kind to identify the dengue endemic regions of the city. Moreover, this study provides a better picture of dengue cases whilst COVID-19 was at its peak. The limitations of this study include a small sample size and a single-centered design. Furthermore, the patients were not followed up to assess the long-term effects of dengue infection.
Conclusion
This study reveals a worrying surge in DF cases in Karachi, especially concentrated in the Korangi district. Out of 159 DENV-positive patients, 73.5% tested positive for NS1 antigen, while 2.6% and 5.3% tested positive for IgM and IgG, respectively. Despite the COVID-19 pandemic, DF demands urgent attention. To effectively combat this growing threat, health authorities must prioritize DF control alongside COVID-19 management. Targeted interventions focused on Korangi and areas with high female populations are crucial. Implementing robust public health actions like mosquito control programs are essential. Furthermore, studies with larger sample sizes and long-term patient follow-up are needed. By taking these decisive steps, we can safeguard the health of Karachi’s residents and effectively manage the rising tide of DF.
Statements
Ethics statement
The studies involving humans were approved by Institutional Review Board (IRB) of Jinnah Postgraduate Medical Center (NO.F.281/2022-GENL/242/JPMC). The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
SM: Supervision and initial conceptualization. MA: Literature search, study design and concept and writeup. HH: Study design and concept, data analysis and data interpretation. All authors participated in the design, interpretation of the studies and analysis of the data and review of the manuscript.
Conflict of interest
The authors declare that they do not have any conflicts of interest.
References
1.
Kyle JL Harris E . Global Spread and Persistence of Dengue. Annu Rev Microbiol (2008) 62:71–92. 10.1146/annurev.micro.62.081307.163005
2.
Bhatt S Gething PW Brady OJ Messina JP Farlow AW Moyes CL et al The Global Distribution and Burden of Dengue. Nature (2013) 496(7446):504–7. 10.1038/nature12060
3.
Haider Z Ahmad FZ Mahmood A Waseem T Shafiq I Raza T et al Dengue Fever in Pakistan: A Paradigm Shift; Changing Epidemiology and Clinical Patterns. Perspect Public Health (2015) 135(6):294–8. 10.1177/1757913915599019
4.
Rana MS Ikram A Alam MM Salman M . Novel Coronavirus Outbreak in Pakistan: Beware of Dengue. J Formos Med Assoc (2021) 120(1):765–6. 10.1016/j.jfma.2020.07.027
5.
Ahmad T Khan NA Rehman MM Jadoon MA . A Story of the Disease Free Area to High Endemic. Bull Environ Pharmacol Life Sci (2014) 3(2):1–4.
6.
ReliefWeb. Pakistan: Dengue Response Emergency Plan of Action (EPoA) DREF Operation N° MDRPK022 - Pakistan (2021). Available From: https://reliefweb.int/report/pakistan/pakistan-dengue-response-emergency-plan-action-epoa-dref-operation-n-mdrpk022 (Accessed January 16, 2022).
7.
WHO. Dengue Fever – Pakistan (2021). Available From: https://www.who.int/emergencies/disease-outbreak-news/item/dengue-fever-pakistan (Accessed January 7, 2022).
8.
ReliefWeb. Pakistan: Dengue Outbreak (2021). Available From: https://reliefweb.int/disaster/ep-2021-000160-pak (Accessed January 16, 2022).
9.
Dussart P Duong V Bleakley K Fortas C Lorn Try P Kim KS et al Comparison of Dengue Case Classification Schemes and Evaluation of Biological Changes in Different Dengue Clinical Patterns in a Longitudinal Follow-Up of Hospitalized Children in Cambodia. PLoS Negl Trop Dis (2020) 14(9):e0008603. 10.1371/journal.pntd.0008603
10.
World Health Organization and UNICEF. Handbook for Clinical Management of Dengue. Geneva, Switzerland: WHO (2012).
11.
De Castro RA De Castro JA Barez MY Frias MV Dixit J Genereux M . Thrombocytopenia Associated With Dengue Hemorrhagic Fever Responds to Intravenous Administration of Anti-D (RH0-D) Immune Globulin. Am J Trop Med Hyg (2007) 76(4):737–42. 10.4269/ajtmh.2007.76.737
12.
Simmons CP Farrar JJ van Vinh Chau N Wills B . Dengue. New Engl J. Med. (2012) 366:1423–32. 10.1056/NEJMra1110265
13.
World Health Organization. Dengue and Severe Dengue (2021). Available From: https://www.who.int/news-room/fact-sheets/detail/dengue-and-severe-dengue (Accessed January 16, 2022).
14.
Aborode AT Corriero AC Fajemisin EA Hasan MM Kazmi SK Olajiga O . Dengue and Coronavirus Disease (COVID-19) Syndemic: Double Threat to an Overburdened Healthcare System in Africa. Int J Health Plann Manage (2021) 37:1851–4. 10.1002/hpm.3334
15.
Haqqi A Awan UA Ali M Saqib MA Ahmed H Afzal MS . COVID‐19 and Dengue Virus Coepidemics in Pakistan: A Dangerous Combination for an Overburdened Healthcare System. J Med Virol (2021) 93(1):80–2. 10.1002/jmv.26144
16.
Khan E Siddiqui J Shakoor S Mehraj V Jamil B Hasan R . Dengue Outbreak in Karachi, Pakistan, 2006: Experience at a Tertiary Care Center. Trans R Soc Trop Med Hyg (2007) 101(11):1114–9. 10.1016/j.trstmh.2007.06.016
17.
World Health Organization. Injuries and Violence (2021). Available From: https://www.who.int/news-room/fact-sheets/detail/injuries-and-violence (Accessed March 19, 2021).
18.
Gubler DJ . Dengue and Dengue Hemorrhagic Fever. Clin Microbiol Rev (1998) 11(3):480–96. 10.1128/CMR.11.3.480
19.
Raza FA Rehman SU Khalid R Ahmad J Ashraf S Iqbal M et al Demographic and Clinico-Epidemiological Features of Dengue Fever in Faisalabad, Pakistan. PLoS One (2014) 9(3):e89868. 10.1371/journal.pone.0089868
20.
Shekhar KC Huat OL . Epidemiology of Dengue/Dengue Hemorrhagic Fever in Malaysia—a Retrospective Epidemiological Study 1973-1987. Part I: Dengue Hemorrhagic Fever (DHF). Asia Pac J Public Health (1992) 6(2):15–25. 10.1177/101053959300600203
21.
Alam H . Female Dengue Patients: Higher Mortality Despite Lower Cases, the Daily Star (2023). Available From: https://www.thedailystar.net/health/disease/news/female-dengue-patients-higher-mortality-despite-lower-cases-3407506 (Accessed: January 05, 2024).
Summary
Keywords
dengue fever, COVID-19, emergency department, tropical diseases, Asia
Citation
Mushtaq S, Abro MT and Hussain Hu (2024) Dengue Cases Presenting to the Emergency Department of a Tertiary Care Hospital in Late 2021: A Cross-Sectional Study in Karachi. Int J Public Health 69:1606753. doi: 10.3389/ijph.2024.1606753
Received
22 October 2023
Accepted
07 February 2024
Published
15 February 2024
Volume
69 - 2024
Edited by
Jean Tenena Coulibaly, Félix Houphouët-Boigny University, Côte d’Ivoire
Reviewed by
Muhammad Adil Rasheed, University of Veterinary and Animal Sciences Lahore, Pakistan
Ugochukwu Anthony Eze, National Postgraduate Medical College of Nigeria, Nigeria
Updates
Copyright
© 2024 Mushtaq, Abro and Hussain.
This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Muhammad Tarish Abro, tarishhameed@gmail.com
This Original Article is part of the Special Issue “Neglected Tropical Diseases During the COVID-19 Pandemic”
Disclaimer
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.