 Change Xiong
Change Xiong Ying Xia
Ying Xia Huihui Chen1
Huihui Chen1- 1School of Public Health, Wuhan University of Science and Technology, Wuhan, Hubei, China
- 2Institute of Nursing Research, Hubei Province Key Laboratory of Occupational Hazard Identification and Control, School of Medicine, Wuhan University of Science and Technology, Wuhan, Hubei, China
Objective: The regional inequality of emergency medicine beds distribution has a great impact on population health as well as the accessibility of emergency services. This study aimed to explore the regional inequality of emergency medicine bed distribution and its influencing factors.
Methods: The Gini coefficient and health resource agglomeration were used to analyze the regional inequality of emergency medicine beds distribution by area from 2012 to 2021 in China. Grey correlation models were used to explore the factors influencing the regional inequality of emergency medicine beds distribution.
Results: From 2012 to 2021, Gini coefficients of emergency medicine beds distribution by geographic in China showed a worsening trend, rising from 0.6229 to 0.6636. The average HRAD index was 3.43 in the east and 0.44 in the west. Population structure factors have the greatest influence on the regional inequality of emergency medicine beds distribution.
Conclusion: Health resources allocation strategy only according to population size should be changed. In formulating policies for emergency medicine beds allocation should take into account population structure, financial structure of expenditure, the inequality of geographical distribution and so on.
Introduction
Ensuring that residents enjoy equal medical services is an important goal for the high-quality development of China’s health system. The emergency medical system is an important high-quality medical resource throughout the world. It generally consists of pre-hospital emergency care, hospital emergency departments and intensive care units in China. Pre-hospital emergency services rely on emergency centers, however, emergency centers are very small amount in a region in China, and people mainly rely on hospital emergency departments for most of their urgent medical needs. As a multifunctional unit, emergency department is not only the core of the emergency medical system, but also plays an important role in the medical system. It shoulders the burden of dealing with acute and critical care, public health emergencies, mass trauma events and natural disasters. The global response to the new crown epidemic has shown that [1] effective and adequate emergency medical resources are essential to minimize the negative impact of an outbreak. A study showed that [2] timely and effective emergency medical services can reduce adult unintentional injury mortality by 80%, pediatric unintentional injury mortality by 60%, and mortality in low- and middle-income countries by 45%. Because China’s hierarchical medical system has not yet been fully established, patients who are unable to receive timely medical care in outpatient clinics choose to visit the emergency department (ED) as a medical-seeking strategy to satisfy their medical needs. The limited medical resources in the ED have led to serious overcrowding problems all the time [3]. There is an empirical evidence that [4] a better bed supply strategy can reduce overcrowding in the emergency department and improve the quality of emergency care.
The implementation of the “Healthy China” strategy had substantially increased the effective supply of medical resources in China. The number of emergency department beds nationwide increased from 25,038 to 52,668 in the past decade. Nevertheless, most of the existing strategies on the allocation of health resources are formulated on the basis of population in China, with less consideration given to geographical distribution. As a result, the distribution of resources shows more equal in terms of population, while inequality still exists among regions. Medical institutions, medical staff and beds, and other medical resources were distributed unequally by geographical with Gini coefficients exceeding 0.7 [5]. This leads to a large number of people living within the county having not enough resources for emergency care and poor access to healthcare [6]. The distribution of emergency care resources also shows urban-rural inequalities, with emergency care resources being particularly scarce in rural areas [7].
Factors affecting inequality in the allocation of healthcare resources are manifold [8, 9] including the system, the market, the economy, health insurance and so on. Some studies have shown that [10] factors such as the quantity of the children and elderly population, government investment in healthcare, the quantity of highly qualified population, healthcare expenditures, and government revenues have a large direct impact on the geographical distribution of health resources. Li et al [11, 12] results also found that economic development, urbanization, population aging, level of financial health expenditure and population size are key factors influencing the geographic distribution of medical resources in China. However, previous studies have not explored in depth the factors influencing the regional inequality of emergency medical resources, and the distribution of emergency medicine beds has a more prominent impact on the effectiveness and quality of emergency department care [7]. Moreover, the rationality of geographic distribution and spatial allocation of emergency care resources play a key role in guaranteeing the spatial accessibility of emergency care resources and reducing the morbidity and mortality rate of the population.
This study analyzes the regional inequity of the distribution of emergency medicine beds in 31 provinces as well as in the eastern, central, and western China from 2012 to 2021, and applies the grey correlation model to assess the influencing factors of regional inequity in the distribution of beds in emergency department. The results of the study help to provide actual evidence for adjusting emergency medicine beds allocation policy to optimize the geographic distribution of emergency medicine beds, which contributes to a balanced layout of high-quality medical resources in China.
Methods
Data Collection
The data were obtained from the 2013–2022 China Statistical Yearbook and China Health Statistical Yearbook, covering 31 provinces, autonomous regions and municipalities directly under the central government in China in this study.
Defining Variables
In this study, we calculated the Gini coefficient of emergency medicine beds by area (per 10,000 km2) and the degree of agglomeration of geographic areas to represent the regional inequity of emergency medicine beds distribution, and explored the factors affecting the regional inequality of emergency medicine beds distribution from the economy, population and medical resources/indicators dimensions. The other control variables were selected and defined as shown in Table 1.
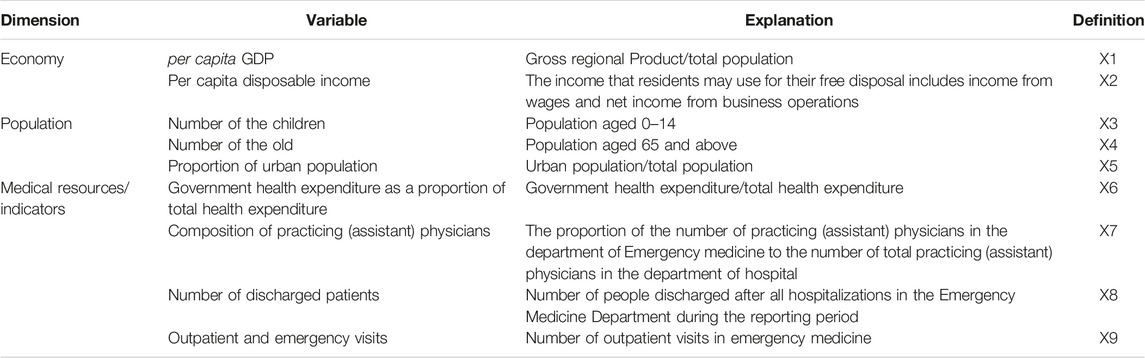
Table 1. Influencing factors of geographic equality of emergency beds. (China, 2012–2021).
Data Analysis
Gini Coefficient
In this study, the Gini coefficient (G) was applied to assess the inequality of the geographic distribution of emergency medicine beds. The closer the value of G is to 1, the more unequal it is. The formula used to calculate G is as follows:
where Wi is the proportion of each province’s geographic area to the total area of the country, Yi is the proportion of emergency medicine beds in each province to the total number of emergency medicine beds in the country, and Vi denotes the cumulative proportion of each indicator in each of the 31 provinces (ranked from smallest to largest in terms of the number of emergency medicine beds per 10,000 square kilometers). n represents the 31 provinces. These data were analyzed using Stata 26.0 and EXCEL 2016.
Health Resource Agglomeration Degree
Health resource agglomeration degree (HRAD) is a new indicator for evaluating the inequality of health resource distribution [13]. This study analyzed the clustering of emergency medicine beds in eastern, central, and western China. The eastern, central, and western regions are based on geographic location and level of economic development. The eastern region includes Hebei, Liaoning, Jiangsu, Zhejiang, Fujian, Shandong, Guangdong, Hainan, Beijing, Tianjin, and Shanghai; the central region includes Shanxi, Jilin, Heilongjiang, Anhui, Jiangxi, Henan, Hubei, and Hunan; and the western region includes Sichuan, Guizhou, Yunnan, Shaanxi, Gansu, Qinghai, Inner Mongolia, Guangxi, Tibet, Ningxia, and Xinjiang and Chongqing [14]. The formula for calculating the degree of agglomeration based on geographic area is:
HRADi denotes the concentration of emergency medicine beds in a region i, HRi denotes the number of emergency medicine beds, and Ai denotes the land area; An is the land area of the region at the upper level, and HRn is the number of emergency medicine beds in the region at the upper level.
Grey Relational Analysis
Grey Relational Analysis (GRA) modeling, is a popular technique for decision analysis under multiple criteria decision making and uncertainty. Deng GRA, absolute GRA, and SS GRA are the three components of the GRA model. In this study, grey correlation analysis model is adopted to explore the impact of each index on emergency medicine bed inequality by region. Gini coefficient of emergency medicine bed by area (per 10,000 km2) from 2012 to 2021 is used to represent its regional inequality. Grey relational gradient (GRG) represents the outcomes of grey relational models. The absolute GRG and SSGRG models have values ranging from zero to one, whereas, Deng GRG has values ranging from 0.5 to 1. It is also considered highly associated if value is near to 1.
The algorithm for computing the Deng GRA is shown below [15].
If X0 = (x0 (1), x0 (2), …, x0 (n)) is the underlying/reference sequence representing the dependent variable and Xi = (xi (1), xi (2), …, xi (n)) is a set of comparison sequences representing the independent variables, a series of operations results in the grey correlation, γ0i or γ (X0, Xi), where ξ ∈ (0, 1) is the discriminant coefficient, the value of which is usually taken as 0.5. k is the sequence number of the data, and i is the number of influencing factors.
The algorithm for computing the absolute GRA is shown below [16].
The Second synthetic GRA (SSGRA) model can be produced by incorporating the given equation.
Whenever a decision-maker seeks an inclusive evaluation that combines the pros of both “Deng’s GRA” and “Absolute GRA” without endorsing one over another and so sets θ at 0.5, we assumed θ at 0.5 for our analysis [17].
Results
Regional Inequality in Emergency Medicine Beds Distribution
The results of the Gini coefficient by area allocation indicated that the overall geographic distribution of emergency beds was in a state of severe inequality from 2012 to 2021, with Gini coefficients above 0.6. The overall trend was increasing, from 0.6229 in 2012 to 0.6636 in 2021 (see Table 2).
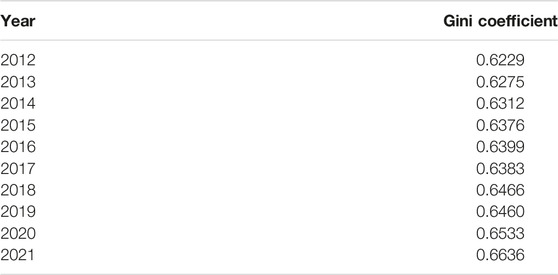
Table 2. Gini coefficients for emergency beds distribution by area. (China, 2012–2021).
From 2012 to 2021, the geographic concentration of emergency medicine beds less than 1 only was in the western China all over the country. The average HRAD index was 3.43 in the east and 0.44 in the west. The geographic clustering of emergency medicine beds in the eastern and central regions is greater than 1, indicating that emergency medicine beds in the eastern and central regions are more equally distributed compared to the western region. Overall, the geographic clustering degree in the eastern and western regions showed a decreasing trend, and the geographic clustering degree in the central region showed an increasing trend (see Table 3). As can be seen from Figures 1, 2, the geographic agglomeration of emergency medicine beds in the eastern region is the largest, with Shandong province and Shanghai city being more prominent. From 2012 to 2021, the emergency medicine beds resources have a tendency to cluster in the central region.
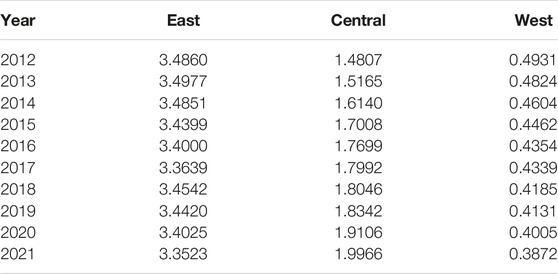
Table 3. Changes in geographic clustering of emergency beds. (China, 2012–2021).
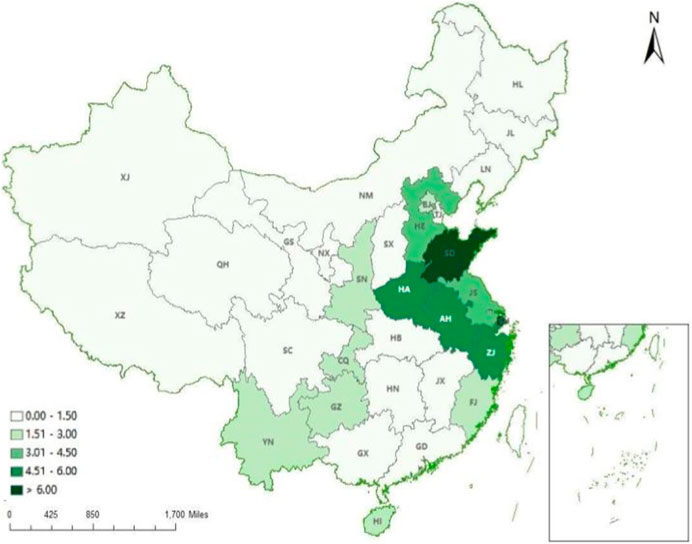
Figure 1. Distribution of regional aggregation of emergency beds in 31 provinces. (China, 2012).
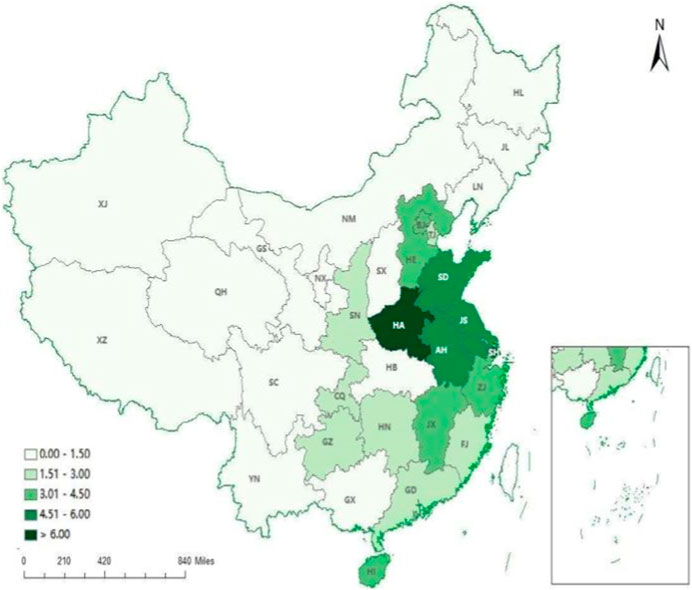
Figure 2. Distribution of regional aggregation of emergency beds in 31 provinces. (China, 2021). Note: BJ, Beijing; TJ, Tianjing; HE, Hebei; SX, Shanxi; NM, Inner Mongoria; SH, Shanghai; JS, Jiangsu; SD, Shandong; ZJ, Zhejiang; AH, Anhui; JX, Jiangxi; FJ, Fujian; GD, Guangdong; GX, Guangxi; HI, Hainan; HA, Henan; HB, Hubei; HN, Hunan; SN, Shaanxi; XJ, Xinjiang; NX, Ningxia; GS, Gansu; QH, Qinghai; CQ, Chongqing; SC, Sichuan; GZ, Guizhou; YN, Yunnan; XZ, Tibet; HL, Heilongjiang; JL, Jilin; LN, Liaoning.
Analysis of Factors Influencing Regional Inequality in Emergency Beds
The results are shown in Table 4. According to the results of Deng’s GRA, the correlation degree of all factors was above 0.5, indicating that all factors were closely related to the geographical inequality of emergency beds. The results of SS GRA were consistent with those of Deng’s GRA. The top three factors were the number of 0–14 children, the composition of practicing (assistant) physicians and the proportion of urban population. The number of outpatient and emergency visits and the per capita disposable income of residents ranked eighth and ninth, respectively. According to the results of absolute correlation, the number of 0–14 children was found to have the strongest effect on regional equality of emergency medicine beds by attaining a grey score of 0.9821. The number of discharged patients and the number of outpatient and emergency patients had the least influence on the regional equality of emergency medicine beds with a grey score of 0.8861 and 0.8693, respectively.
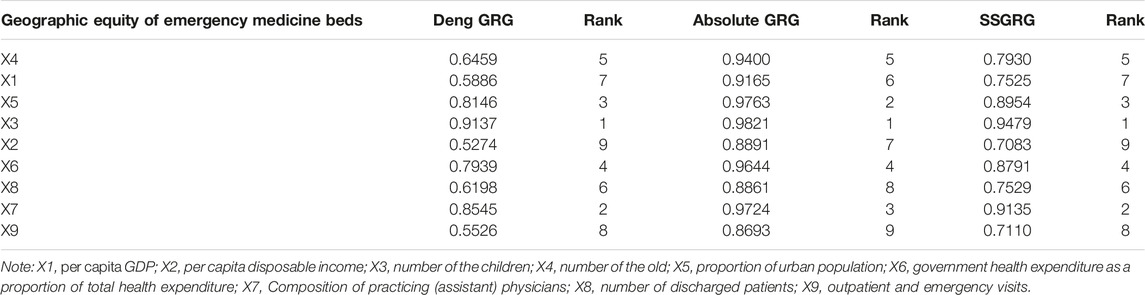
Table 4. Grey correlation evaluation results. (China, 2012–2021).
Discussion
This study depicts provincial inequalities in the distribution of emergency medicine beds by geographic area, assesses and compares the extent to which population, economic, and medical resource factors are associated with regional inequality in emergency medicine beds, and provides a reference for regional allocation of emergency medicine beds. The results of our analysis report the following four key findings.
Regional Inequities in Emergency Medicine Beds Show a Gradual Increasing Trend, 2012–2021
There are obvious regional differences in the overall distribution of emergency medicine beds from 2012 to 2021. Emergency medicine beds are mainly concentrated in the economically developed eastern region, while the distribution of emergency medicine beds in the relatively underdeveloped western region is obviously insufficient. The result is consistent with the results of the overall allocation of health resources [18]. Moreover, the inequality in the geographic distribution of emergency medicine beds has shown a trend of gradual deterioration. This may be attributed to China’s health resource allocation policy. For a long time, the Chinese government allocated health resources mainly according to the living population. The result of this health policy is that equality in health resources is better distributed by population than by geographic area [19]. However, this allocation strategy neglects the special characteristics of remote areas. The number of people living in remote areas is small, the allocation of medical resources according to population is correspondingly small. This leads to the scattered residents will not be able to obtain timely emergency services due to the large geographic area of the province.
Distribution of emergency medicine beds according to geographic shows poor equality and needs more attention. Especially for sparsely populated provinces with large geographic areas, it is an important strategy allocating resources by area to promote the accessibility and equality of health services for the population. Some countries have adopted the allocation of medical resources according to area. For example, the government of Japan [20] had set up a three-tier healthcare medical circle based on geographical characteristics and demand for health services, with strict control over the number of health institutions and hospital beds. In Singapore [21], all public medical institutions are divided into two medical groups, one in the east and the other in the west, according to their geographical location and size. The allocation of emergency medicine beds needs to take into account geographic size, not just the residential population, and the trend of worsening geographic inequality is likely to continue if the allocation strategy is not changed.
Population Structure Factors Are the Most Significant Factors Influencing Regional Inequality in the Distribution of Emergency Medicine Beds
The grey correlations showed that population structure factors has a greatest impact on the regional inequality of emergency medicine department beds, which is consistent with the findings of Wu et al [5]. Children and the elderly population, who are physically weaker due to age, tend to be at higher risk of acute illness and injury, and have a greater need for emergency care. The health problem of left-behind children in rural or remote areas deserves attention, and as a vulnerable group in terms of health, they may need more emergency medical resources to meet their complex medical needs [22]. Some findings [23] have demonstrated that the more adequate emergency medical resources such as beds, the lower the risk of adverse outcomes for elderly patients.
There is a correlation between the proportion of urban population and the regional inequality of emergency medicine beds. Since the reform and opening up, the acceleration of urbanization has created difficulties in the reasonable distribution of medical resources [24]. The gap is widening between urban and rural areas in terms of the supply of health resources and the demand for health services. High-quality emergency medical resources are mainly concentrated in large hospitals in big cities, which may be related to the “siphoning effect” on emergency medical resources as to the high population density of urban areas [22]. Overall, multiple population factors can influence the regional inequality of emergency medicine beds.
Increasing Government Health Expenditure as a Proportion of Total Health Costs Is Beneficial to Reducing Regional Inequalities in the Distribution of Emergency Medicine Beds
The results indicated expanding government’s health spending’s share of total health costs rather than only increasing government’s health spending in order to have a mitigating effect on regional inequality in acute care bed. This is in consistent with the findings of Cashin et al [25]. The government’s ability to utilize its finances has a significant impact on the distribution of health resources, and it is necessary to attach great importance to building financial capacity in the allocation of health resources. Poor areas are often less likely to have adequate access to emergency care than wealthier areas. There is a significant gap in the equality of medical resource distribution among provinces. The scarcity and uneven distribution of emergency care resources is also a serious problem in low- and middle-income countries [26]. Increasing the proportion of government health expenditures can strengthen the construction of medical facilities in remote and underdeveloped provinces and reduce the gap in the distribution of emergency medicine beds among provinces.
In a word, local governments should optimize the structure of financial expenditure, increase the proportion of government health expenditure in the total cost of health, expand the coverage of emergency medical resources, and decrease the inequality in the regional distribution of emergency medicine beds.
The Composition of Practicing (Assistant) Physicians Is Closely Related to the Regional Inequality of Emergency Medicine Beds Distribution
The findings showed that the composition of practicing (assistant) physicians in the emergency medicine department was strongly associated with the inequality of the geographic distribution of beds. The study of Horev T et al supported our findings [27]. Licensed (assistant) physicians play a more prominent role as an integral part of the acute care delivery system [28]. The distribution of practicing (assistant) physicians in the emergency department will have an impact on the effectiveness, accessibility and sustainability of emergency medical services. However, the western region lags behind in terms of environmental conditions, economic level and compensation compared with the central and eastern regions, the trend of physician mobility is more urban-centered, which will exacerbate the geographic inequality in the allocation of beds [5]. The government needs to make targeted plans and strategies in undeveloped provinces to reduce geographic inequalities in the distribution of emergency department physicians and beds and to narrow the gap in the level of emergency medical services among regions.
Conclusion
Gradual deterioration in the inequality of regional distribution of emergency medicine beds in China from 2012 to 2021. Three factors, population structure, economy level and medical resources/indicators had different influence on the disparity of emergency medicine beds distribution, and the population structure having the greatest degree of association with the regional inequality of emergency medicine beds. The government should consider the inequality of geographical distribution when formulating resource allocation policies and optimize financial structure expenditures. In undeveloped areas, it is important to take practical and feasible simulation measures to increase the number of emergency physicians. In regions with a high proportion of vulnerable populations such as the elderly and children, or a high proportion of the urban population, the number of emergency medicine beds should be increased.
Enlightenment
The results of this study provide a basis for promoting the geographic equality, service accessibility and sustainable development of emergency medical resources in developing countries. We call on countries around the world to pay great attention to the spatial inequality of emergency medical resources to improve the emergency medical service system accessibility. This study suggests that both population equity and spatial accessibility equity should be considered simultaneously in the practice of allocation of emergency medicine beds. Moreover, in areas where spatial distribution of emergency medicine beds is unequitable but the distribution is equitable according to population, priority should be given to reducing spatial distribution unfairness in emergency medical resource planning. Conversely, priority should be given to reducing population distribution unfairness.
Limitation and Future Research
This is an exploratory study only explored the association between macro factors such as population, economy, and medical factors and regional inequality of emergency medicine beds distribution. In the future, attention could be paid to the interaction between other factors such as individual aspects and macro influences. In addition, Due to the availability of data, this study did not test the results robust of grey correlation analysis. Future studies should consider more factors and use more complete database to comprehensively evaluate the distribution of emergency medicine beds.
Data Availability Statement
The survey data collected and analyzed during the current study are available from the corresponding author on reasonable request.
Author Contributions
CX designed the study. YX analyzed the data and wrote the manuscript. HC assisted the analysis and revised the manuscript. CX, YX, and JC participated in data interpretation. All authors contributed to the article and approved the submitted version.
Funding
This study was funded by the Humanity and Social Science Foundation from Ministry of Education of China (23YJAZH166).
Conflict of Interest
The authors declare that they do not have any conflicts of interest.
Acknowledgments
This paper cited the China Health Statistical Yearbooks and China Statistical Yearbooks, which provide the data for this study.
References
1. Wang, X, Wu, W, Song, P, and He, J. An International Comparison Analysis of Reserve and Supply System for Emergency Medical Supplies Between China, the United States, Australia, and Canada. Biosci Trends (2020) 14:231–40. doi:10.5582/bst.2020.03093
2. Wong, HT, Lin, TK, and Lin, JJ. Identifying Rural-Urban Differences in the Predictors of Emergency Ambulance Service Demand and Misuse. J Formos Med Assoc (2019) 118:324–31. doi:10.1016/j.jfma.2018.05.013
3. Tsai, JCH, Weng, SJ, Liu, SC, Tsai, YT, Gotcher, DF, Chen, CH, et al. Adjusting Daily Inpatient Bed Allocation to Smooth Emergency Department Occupancy Variation. Healthcare (Basel) (2020) 8:78. doi:10.3390/healthcare8020078
4. Khare, RK, Powell, ES, Reinhardt, G, and Lucenti, M. Adding More Beds to the Emergency Department or Reducing Admitted Patient Boarding Times: Which Has a More Significant Influence on Emergency Department Congestion? Ann Emerg Med (2009) 53:575–85. doi:10.1016/j.annemergmed.2008.07.009
5. Wu, X, Zhang, Y, and Guo, X. Research on the Equity and Influencing Factors of Medical and Health Resources Allocation in the Context of COVID-19: A Case of Taiyuan, China. Healthcare (Basel) (2022) 10:1319. doi:10.3390/healthcare10071319
6. Neville, S, Napier, S, Adams, J, and Shannon, K. Accessing Rural Health Services: Results From a Qualitative Narrative Gerontological Study. Australas J Ageing (2020) 39:e55–e61. doi:10.1111/ajag.12694
7. Jin, K, Zhang, H, Seery, S, Fu, YY, Yu, SS, Zhang, LL, et al. Comparing Public and Private Emergency Departments in China: Early Evidence From a National Healthcare Quality Survey. Int J Health Plan M (2020) 35:581–91. doi:10.1002/hpm.2968
8. Shi, BG, Fu, YT, Bai, XD, Zhang, XY, Zheng, J, Wang, YP, et al. Spatial Pattern and Spatial Heterogeneity of Chinese Elite Hospitals: A Country-Level Analysis. Front Public Health (2021) 9:710810. doi:10.3389/fpubh.2021.710810
9. Love-Koh, J, Griffin, S, Kataika, E, Revill, P, Sibandze, S, and Walker, S. Methods to Promote Equity in Health Resource Allocation in Low- and Middle-Income Countries: An Overview. J Glob Health (2020) 16:6. doi:10.1186/s12992-019-0537-z
10. Zhou, Y, Zhao, K, Han, J, Zhao, S, and Cao, J. Geographical Pattern Evolution of Health Resources in China: Spatio-Temporal Dynamics and Spatial Mismatch. Trop Med Infect Dis (2022) 7:292. doi:10.3390/tropicalmed7100292
11. Guo, QB, Luo, K, and Hu, RD. The Spatial Correlations of Health Resource Agglomeration Capacities and Their Influencing Factors: Evidence From China. Int J Env Res Pub Health (2020) 17:8705. doi:10.3390/ijerph17228705
12. Li, J, Chen, X, Han, X, and Zhang, G. Spatiotemporal Matching Between Medical Resources and Population Ageing in China From 2008 to 2017. BMC Public Health (2020) 20:845. doi:10.1186/s12889-020-08976-z
13. Chen, J, Lin, ZC, Li, L, Wang, YY, Pan, Y, Yang, J, et al. Ten Years of China’s New Healthcare Reform: A Longitudinal Study on Changes in Health Resources. BMC Public Health (2021) 21:2272–13. doi:10.1186/s12889-021-12248-9
14. Dai, G, Li, R, and Ma, S. Research on the Equity of Health Resource Allocation in TCM Hospitals in China Based on the Gini Coefficient and Agglomeration Degree: 2009-2018. Int J Equity Health (2022) 21:145. doi:10.1186/s12939-022-01749-7
15. Liu, SF, Zhang, HY, and Yang, YJ. Explanation of Terms of Grey Incidence Analysis Models. Grey Syst (2017) 7:136–42. doi:10.1108/gs-11-2016-0045
16. Liu, SF, Xie, NM, and Forrest, J. Novel Models of Grey Relational Analysis Based on Visual Angle of Similarity and Nearness. Grey Sys (2011) 1:8–18. doi:10.1108/20439371111106696
17. Rehman, E, and Rehman, S. Particulate Air Pollution and Metabolic Risk Factors: Which Are More Prone to Cardiac Mortality. Front Public Health (2022) 10:995987. doi:10.3389/fpubh.2022.995987
18. Li, Z, Yang, L, Tang, S, and Bian, Y. Equity and Efficiency of Health Resource Allocation of Chinese Medicine in Mainland China: 2013-2017. Front Public Health (2020) 8:579269. doi:10.3389/fpubh.2020.579269
19. Yao, H, Zhan, C, and Sha, X. Current Situation and Distribution Equality of Public Health Resource in China. Arch Public Health (2020) 78:86. doi:10.1186/s13690-020-00474-3
20. Ishikawa, T, Nakao, Y, Fujiwara, K, Suzuki, T, Tsuji, S, and Ogasawara, K. Forecasting Maldistribution of Human Resources for Healthcare and Patients in Japan: A Utilization-Based Approach. BMC Health Serv Res (2019) 19:653. doi:10.1186/s12913-019-4470-x
21. Lim, MK. Shifting the Burden of Health Care Finance: A Case Study of Public-Private Partnership in Singapore. Health Policy (2004) 69:83–92. doi:10.1016/j.healthpol.2003.12.009
22. Yang, C, Cui, D, Yin, S, liu, X, Yang, Y, Ke, X, et al. Fiscal Autonomy of Subnational Governments and Equity in Healthcare Resource Allocation: Evidence From China. Front Public Health (2022) 10. doi:10.21203/rs.3.rs-1765344/v1
23. Ukkonen, M, Jamsen, E, Zeitlin, R, and Pauniaho, SL. Emergency Department Visits in Older Patients: A Population-Based Survey. BMC Emerg Med (2019) 19:20. doi:10.1186/s12873-019-0236-3
24. Du, M, Zhao, Y, Fang, T, Fan, L, Zhang, M, Huang, H, et al. Evaluating the Inequality of Medical Resource Allocation Based on Spatial and Non-Spatial Accessibility: A Case Study of Wenzhou, China. Sustainability (2022) 14:8331. doi:10.3390/su14148331
25. Cashin, C, and Gatome-Munyua, A. The Strategic Health Purchasing Progress Tracking Framework: A Practical Approach to Describing, Assessing, and Improving Strategic Purchasing for Universal Health Coverage. Health Syst Reform (2022) 8:e2051794. doi:10.1080/23288604.2022.2051794
26. Ouma, PO, Maina, J, Thuranira, PN, Macharia, PM, Alegana, VA, English, M, et al. Access to Emergency Hospital Care Provided by the Public Sector in Sub-Saharan Africa in 2015: A Geocoded Inventory and Spatial Analysis. Lancet Glob Health (2018) 6:e342–50. doi:10.1016/S2214-109X(17)30488-6
27. Horev, T, Pesis-Katz, I, and Mukamel, DB. Trends in Geographic Disparities in Allocation of Health Care Resources in the US. Health Policy (2004) 68:223–32. doi:10.1016/j.healthpol.2003.09.011
Keywords: regional inequality, emergency medicine beds, resources distribution, associated factors, Gini coefficient
Citation: Xiong C, Xia Y, Chen H and Cheng J (2024) Regional Inequality and Associated Factors of Emergency Medicine Beds Distribution in China. Int J Public Health 69:1606812. doi: 10.3389/ijph.2024.1606812
Received: 05 November 2023; Accepted: 06 March 2024;
Published: 08 April 2024.
Edited by:
Nino Kuenzli, Swiss Tropical and Public Health Institute (Swiss TPH), SwitzerlandReviewed by:
Martin Dlouhy, University of Economics, CzechiaLaura Acosta, CCT CONICET Córdoba, Argentina
Copyright © 2024 Xiong, Xia, Chen and Cheng. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Change Xiong, xche77@163.com